
Presentation
Known case of pulmonary tuberculosis presented with recent onset of severe chest pain and dyspnea after chest intubation.
Patient Data
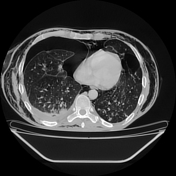


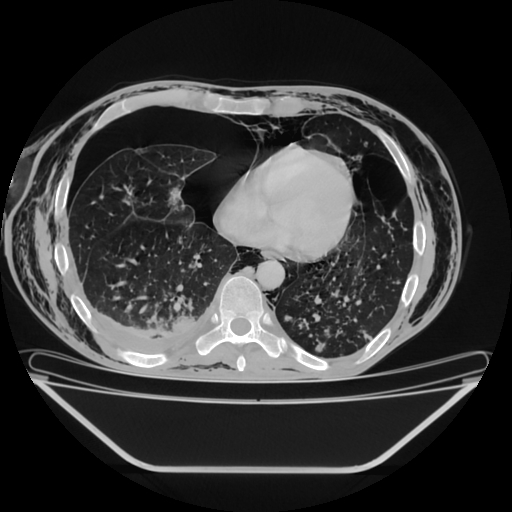
Right hydropneumothorax with atelectasis of the lower lobe and partial collapse of the ipsilateral upper lobe. A chest tube is located in 5th ICS.
Extensive subcutaneous emphysema dissecting into the deeper soft tissue and musculature, extending from chest wall to mediastinum and neck spaces bilaterally.
Large coalescing cavitating lesions, cystic bronchiectasis and parenchymal fibrosis noted in bilateral upper lobes signifies sequelae of chronic infection. And areas of patchy ground glass attenuation with centrilobular branching nodules (tree in bud) are seen in the posterior basal segment of left lower lobe. Mild left side pleural effusion is present.
Case Discussion
Subcutaneous emphysema is a well-known, dangerous and avoidable cause of increased morbidity and mortality. It is not only associated with pneumothorax but also poor intubation technique, tube blockage, anchorage and side port migration into subcutaneous tissue.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.