
Presentation
Tachypnea, cough and fever.
Patient Data

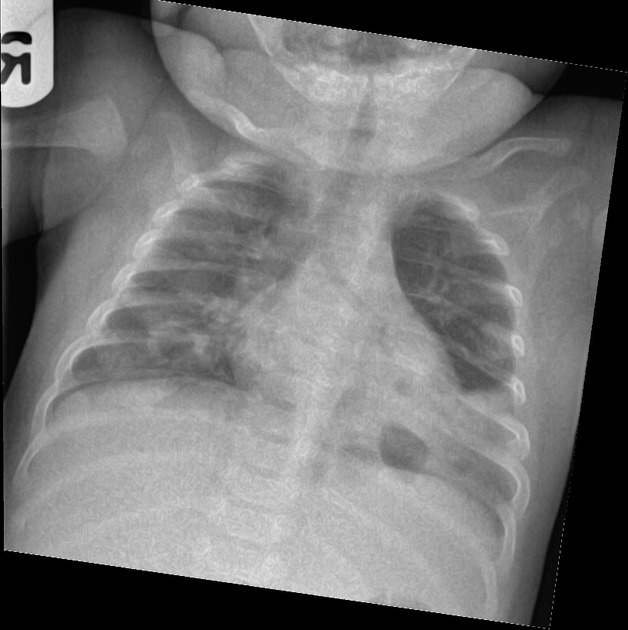
Initial airspace opacity in both lower zones, more extensive on the left.
Given the history and imaging findings, the patient was treated for pneumonia. Symptoms were slow to resolve with treatment and progress images demonstrate development of thin walled cystic spaces in both lower zones.
One week after initial image, thick-walled cystic spaces have developed within the bibasal airspace opacity.
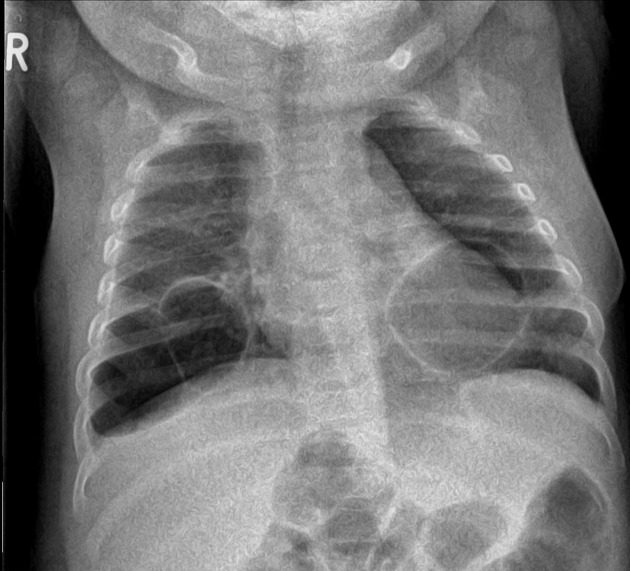
Two months after initial examination, the airspace opacities have resolved and thin-walled cystic spaces have developed bi-basally, consistent with post pneumonic pneumatoceles.
Case Discussion
The following theories have been proposed as to the mechanism of post pneumonic pneumatocele formation; however, the exact mechanism remains controversial.
1. The initial event is inflammation, with narrowing of the bronchus, leading to the formation of an endobronchial ball valve. Ultimately, this bronchial obstruction leads to the distal dilatation of the bronchi and alveoli.
2. A peribronchial abscess forms and subsequently ruptures its contents into the bronchial lumen. This also acts similarly to a ball-valve obstruction in the bronchus and leads to distal dilatation.
3. Pneumatoceles are caused by bronchial inflammation that ruptures the bronchiolar walls and causes the formation of "air corridors." Air dissects down these corridors to the pleura and forms pneumatoceles, a form of subpleural emphysema.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.