
Presentation
Abdominal pain and vomiting beginning approximately 4 hours prior to initial imaging.
Patient Data




CT performed outside the hospital demonstrated ileocolic intussusception extending to the right upper quadrant, shows telescoping bowel with intussusception extending to the hepatic flexure.

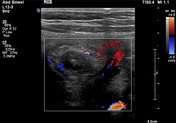

Target sign in the right upper quadrant transverse colon verified continued presence of intussusception after patient transfer. Preserved blood flow within the intussusceptum.

Water-soluble contrast enema reduction of intussusception.
Rounded filling defect with meniscus of contrast at the hepatic flexure. This progressively reduced to the ileocecal valve with contrast filling the appendix. However, there initially remained a small amount of fullness at the ileocecal valve without reflux of contrast into the ileum. Eventually, there was reflux of contrast into the ileum with reduction of the small residual filling defect at the ileocecal valve.
Case Discussion
The patient's vague clinical presentation at the outside hospital triggered evaluation with CT rather than the typical workup of ultrasound. Approximately 5 hours later when the patient arrived, ultrasound confirmed continued presence of the intussusception and preserved vascularity. Immediately after ultrasound, the patient was taken for enema reduction, which was successful on the second attempt. (The intussusception easily reduced to the level of the ileocecal valve initially but would not easily reflux on the first attempt, as commonly happens).


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.