
Presentation
Pain inferior to the right clavicle.
Patient Data
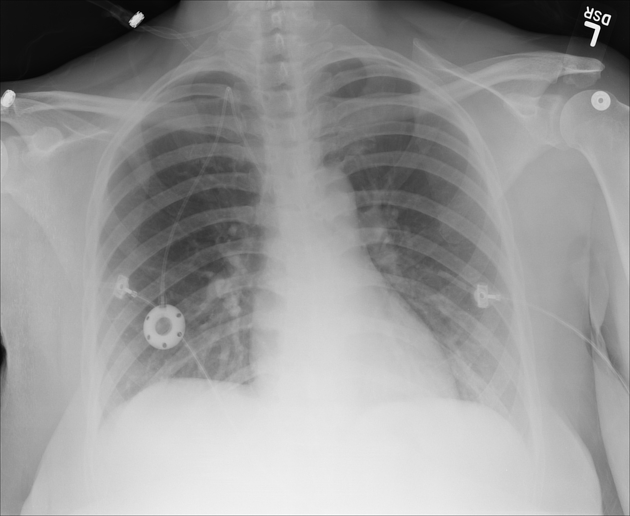
There is a normal cardiomediastinal silhouette with lungs expanded equally bilaterally. The trachea is midline. No pneumothorax, pleural effusion, infiltrate, or mass is seen. The osseous structures are intact. The soft tissues are unremarkable. Right chest Port-a-Cath with the tip within the proximal SVC.

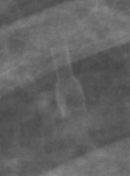
Post port removal from the right anterior chest wall. The retained connecting-hub of the Port-a-Cath can be visualized at the right 7th rib.
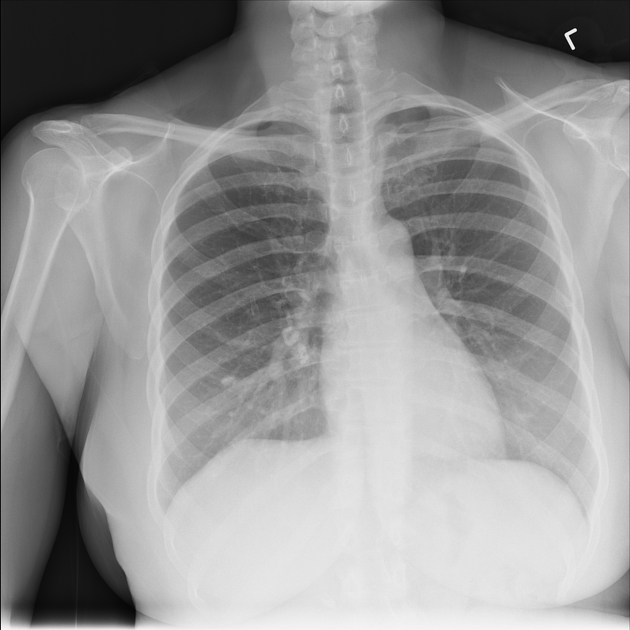
The cardiomediastinal silhouette is normal. Calcified right hilar lymph nodes are noted, along with a calcified granuloma in the right lung. There is no focal consolidation, pleural effusion or pneumothorax. The lungs are well inflated. Pulmonary vascularity is normal. Imaged osseous structures are intact.
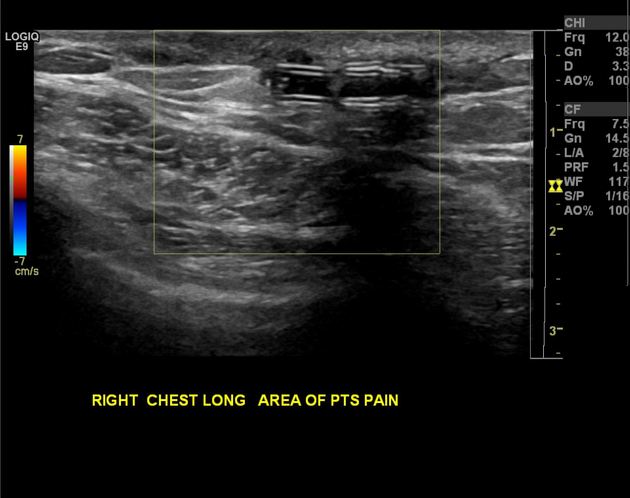
There is a 1.5 cm long fragment of retained tubing within the soft tissues of the right anterior chest wall. This finding is consistent with the piece of connecting tubing used to secure the catheter to the Port-a-Cath reservoir. Note is made of surrounding scar tissue. However, there is no abscess formation.
Case Discussion
Upon removal of the Port-a-Cath, the connecting hub was left behind. Ultrasound confirmed the finding a few days later and it was excised out. The hub was initially not detected on the plain radiograph.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.