
Presentation
Biopsy of suspicious lung lesion. Asymptomatic.
Patient Data
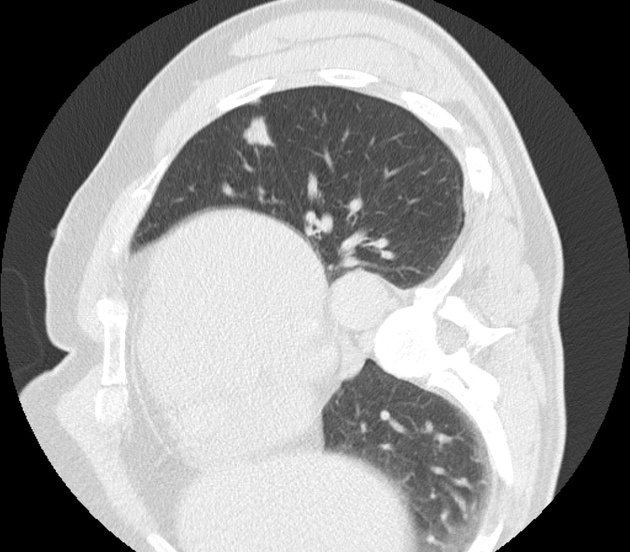
A suspicious lung nodule is seen in the left upper lobe adjacent to the oblique fissure and is targeted for biopsy with the patient in right lateral decubitus position.
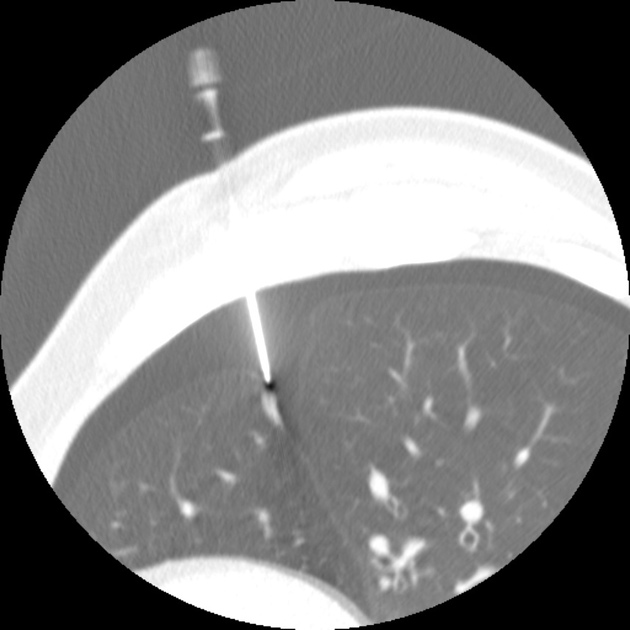
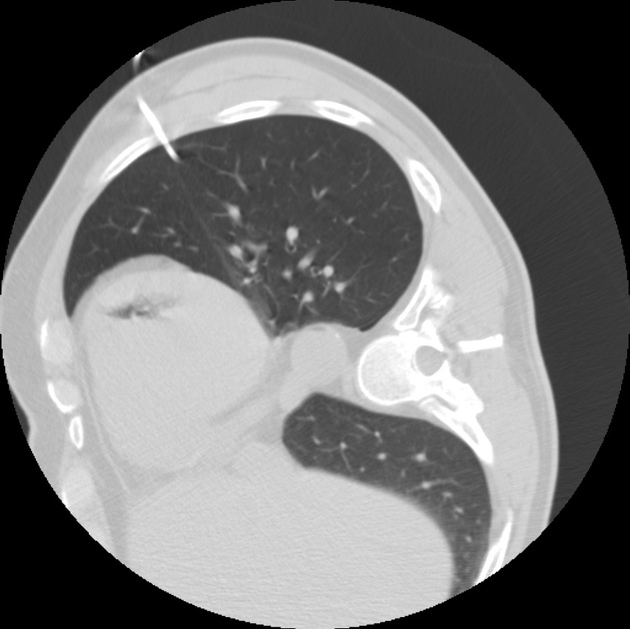
The suspicious lung nodule was successfully biopsied by a transthoracic technique (partially shown here because of needle angulation). An iatrogenic pneumothorax has occurred.
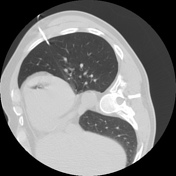

Post-biopsy, a chest tube was inserted via Seldinger technique because the patient was moderately symptomatic from his iatrogenic pneumothorax. However (and this was initially missed in the heat of the action) there is now air in the left ventricule and a small air crescent in the aorta, corresponding to an iatrogenic systemic arterial air embolism.
Case Discussion
Systemic air embolism (air in the systemic arterial circulation) is considered a rare complication of CT-guided percutaneous lung biopsy. Though often self-limiting, it can lead to disastrous, even fatal complications when the air embolus reaches the brain or coronary arteries.
Different methods have been advocated to reduce the risk of this complication, one of which is placing the patient so that the lesion to be biopsied lies below the left atrium 3.
If an air embolus is identified, treatment should included 100% oxygen and close monitoring. Depending on the symptoms, hyperbaric oxygen chamber therapy might be indicated. Some have advocated placing the patient in a right decubitus Trendelenburg position in the hopes of keeping the air in the apex of the left ventricle so it does not embolize further in the arterial circulation.
In this specific case, the air was only noted the next morning upon reviewing the images to finalize the report. The referring physician was contacted, who confirmed that the patient was completely asymptomatic neurologically and from a respiratory perspective. Prudently, a follow-up scan was ordered which showed complete resolution of the air embolus.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.