
Presentation
Abdominal lymphadenopathy and a pancreatic mass detected on ultrasound
Patient Data









Chest
Lungs and large airways: a 13 x 9.5 mm fairly well defined parenchymal lesion is seen sitting on the major fissure inside the apical segment of left lower lobe. No other lung lesions.
Pleura: normal. No pleural effusion or thickening.
Heart and pericardium: heart size is normal. Cardiac motion artefacts present, however increased prominence of left ventricle papillary muscles.
Mediastinum and hila: enlarged, right upper and left upper paratracheal, aortopulmonary, subcarinal and right hilar stations largest 16 mm in short axis.
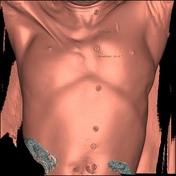
Chest wall and lower neck: Non visualization of right pectoralis major and minor. Mild hypoplasia of right lower half of manubrium with inward flexion of manubrium.
Vessels: normal.
Bones: mild dorsal spondylosis.
Abdomen and pelvis
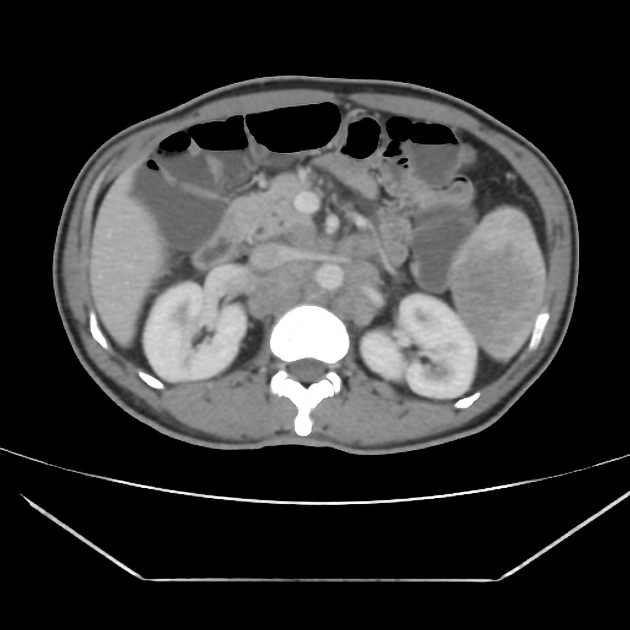
Numerous enlarged solid lymph nodes both discrete and in sheet forms are seen in retroperitoneum – para aortic, aorto caval and para caval stations, along celiac axis and splenic vein and also in right external iliac group largest 3 cm in short axis.
Liver: mildly enlarged. No focal lesions.
Bile ducts: normal
Gall bladder: no calcified stones. Normal caliber wall.
Pancreas: normal in morphology. 3.0 x 2.0 cm poorly defined lesion in tail. Normal head, uncinate process and body. Normal pancreatic duct.
Spleen: enlarged, 13 cm with multiple parenchymal hypodense infiltrates, largest 5.0 x 4.0 cm in lower pole.
Adrenals: normal
Kidneys: normal
Bowel: normal caliber and morphology. No focal lesions.
Peritoneum: no ascites or free air; no fluid collection.
Vessels: normal.
Abdominal wall: normal.
Urinary bladder: circumferential mural thickening and poor distension. No calculi
Prostate: normal.
Diffuse calcification of bilateral seminal vesicles and vas deferens.
Bones: mild lumbar spondylosis.
Case Discussion
This patient came to us for evaluation of the pancreas for a pancreatic lesion detected on ultrasound. What we did not expect was to find the absence of the right pectoralis major and minor. Hepatosplenomegaly with asymmetrically more abdominal lymphadenopathy, appearing as sheet like masses in the retroperitoneum, encasing and displacing blood vessels. There is sheet like lymph node enlargement along the splenic vein also giving a encased appearance to the pancreas.
Associations of Poland syndrome with leukemias and lymphomas have been documented earlier.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.