
Presentation
Chest tightness and shortness of breath.
Patient Data
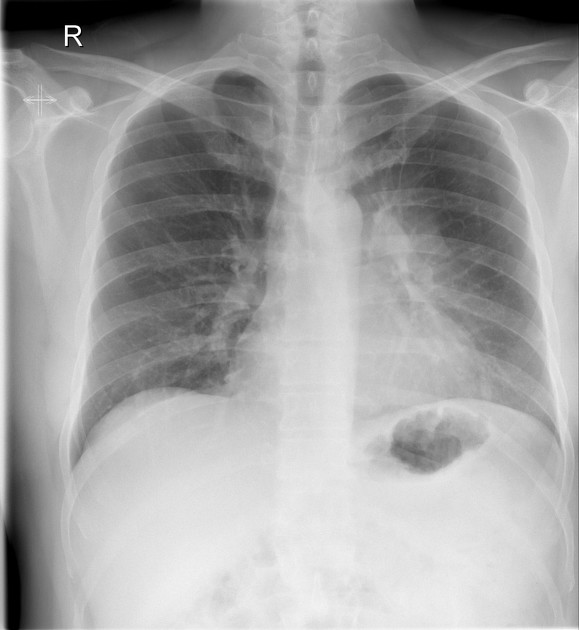
Luftsichel sign suggestive of left upper lobe collapse.




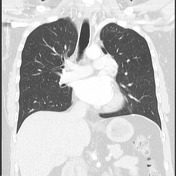



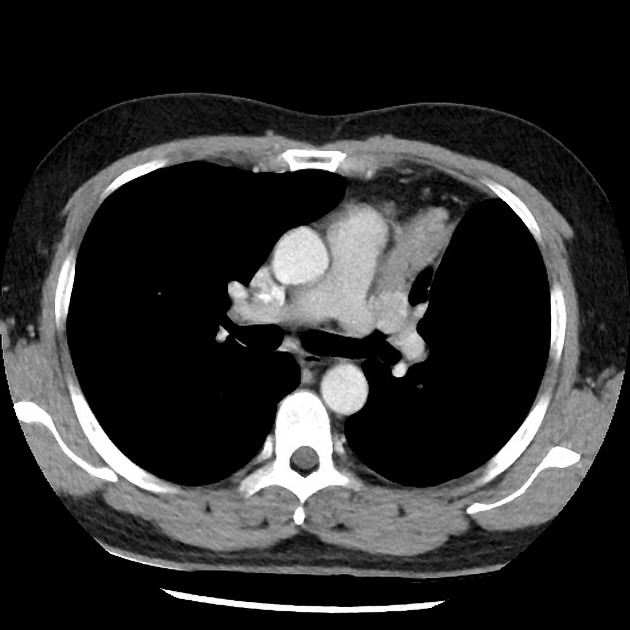
There is a well-defined 3.2 cm hypervascular mass within the bronchus to the left upper love causing its collapse. No enlarged mediastinal lymph nodes or other suspicious lesions. Bilateral gynecomastia.
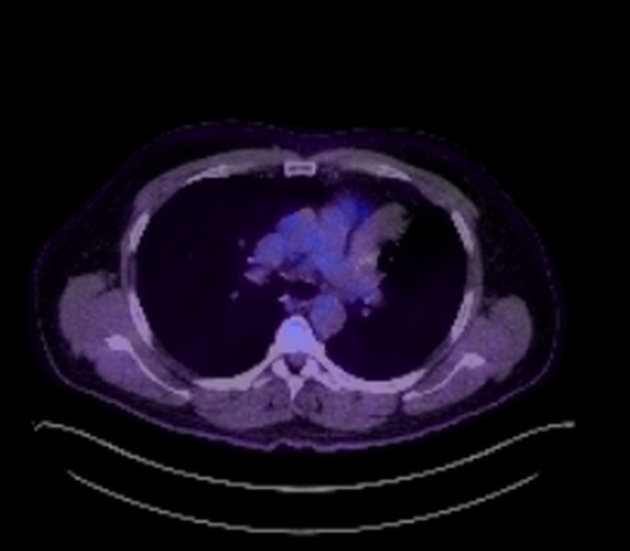
No FDG avidity of the bronchial mass. No abnormal avidity elsewhere.

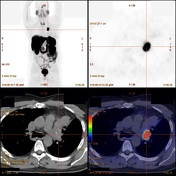
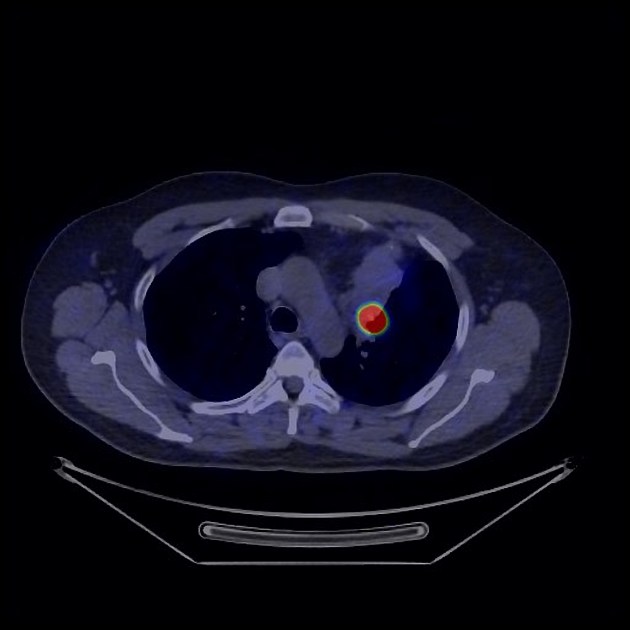
Strong Dotatate avidity of the bronchial mass. No abnormal avidity elsewhere.
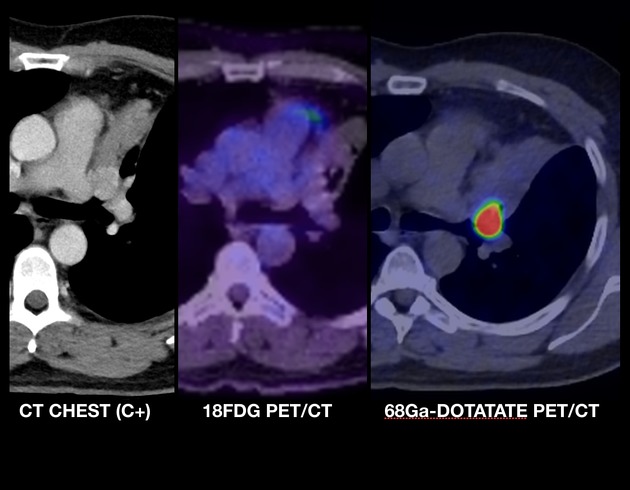
side by side: hypervascular endobronchial lesion with low FDG and high Dotatate uptake.
Macroscopy: 1. Labeled "Left upper lobe resection". Left upper lobectomy specimen, 140 x 76 x 43 mm, 145 g. At the bronchial resection margin, inked green, there is a 31 x 26 x 23 mm tumor that is pale green and uniform. The tumor distends and fills the bronchial airways, and protrudes out of the bronchial resection margin. The closest point of tethering is 2 mm from the resection margin. The tumor is less than 1 mm from the lung parenchymal resection margin. No invasion of parenchyma is demonstrated. The tumor obstructs the left upper lobe bronchus at the hilum, with bronchiectasis of the inferior segmental airways. The background lung is brown, spongy and soft.
2. Labeled "Station 7 node". Yellow, fatty tissue, 21 x 9 x 8 mm, containing one black lymph node, 12 mm.
Tumor is present within the lumen of the left upper lobe bronchus at the resection margin, however, the point of tumor attachment to the bronchial wall is 2 mm clear of the resection margin.
Microscopy: 1. The lumen of the left upper lobe bronchus. The tumor is composed of a trabecular proliferation of relatively uniform cells that have round nuclei, stippled chromatin, and a moderate amount of granular cytoplasm. No mitotic figures are seen (0 per 10 HPF), and there is no tumor necrosis. No lymphovascular or perineural invasion seen. Distal to the tumor, there is bronchial dilation with inspissation of mucus. Away from the tumor, the alveolar architecture is preserved with small numbers of intra-alveolar macrophages.
2. Sections show lymph node with reactive histiocytosis and mild anthracosis. There is no malignancy.
Case Discussion
Typical presentation of a central bronchial carcinoid tumor with upper lobe collapse.
This case has been radiologically staged (IASLC 8th edition) as T2a, N0, and M0. Further confirmed in the resection.
Note that the CT features are those of a well-defined hypervascular endobronchial mass and are already highly suggestive of a neuroendocrine tumor. Given these tumors have a low metabolic activity while well-differentiated early stages, they commonly are 18F-FDG negative on PET/CT. Whereas on PET/CT performed with 68Ga-DOTATATE, they have high uptake because due to their significant somatostatin receptors (SSR2) expression. On the other hand, in advanced stages, where tumors are more poorly differentiated, this pattern of uptake will invert, showing high 18F-fluorodeoxyglucose and low 68Ga-DOTATATE avidity 1.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.