
Presentation
Abdominal pain. Known to the gastroenterology clinic.
Patient Data
Age: 40 years
Gender: Male
Download
Info

Small bowel gaseous dilatation and signs of extensive likely bowel surgery in the pelvis. No evidence of gas in the large bowel (procto-colectomy?). No pneumoperitoneum.




Download
Info
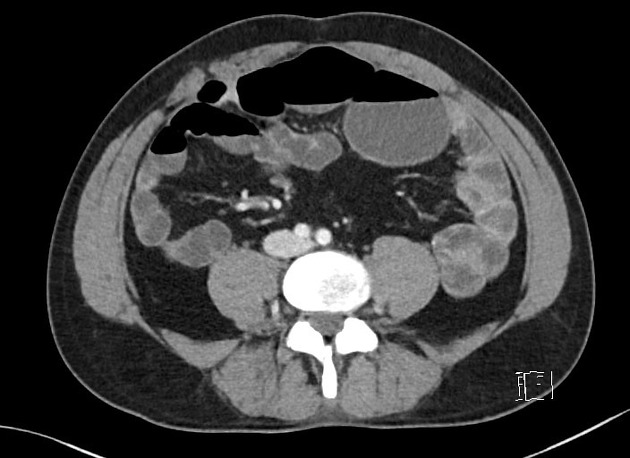
Features of proctocolectomy with ileal pouch-anal anastomosis (IPAA) and a short segment of active ileal inflammation with stricture in its afferent loop. Engorged vasa recta. No signs of penetrating disease. The bowel is otherwise unremarkable.
Case Discussion
This patient has a known history of Crohn's disease and has had proctocolectomy with ileal pouch-anal anastomosis many years ago (J-pouch surgery). Features are those of active Crohn's information with stricture.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.