
Presentation
Abdominal pain and distension of about 3 months duration. Recent vaginal purulent discharge.
Patient Data


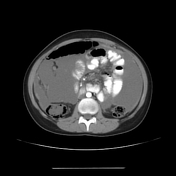


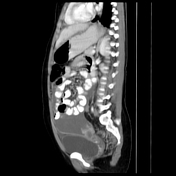
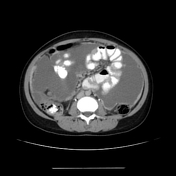
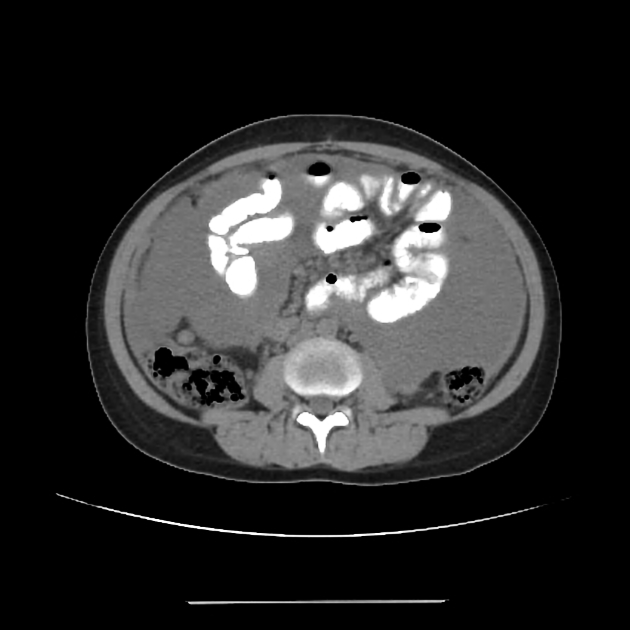
Extensive diffuse peritoneal nodular thickening and enhancement, associated with a moderate amount of ascites. Thickening and stranding throughout the lower abdominal omentum. Multiple enlarged cystic necrotic right iliac mesenteric lymph nodes. Mild mural thickening and enhancement of the terminal ileum is noted.
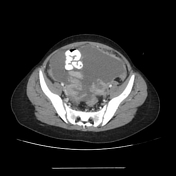
Bilateral large irregular, multilocular enhancing adnexal cystic lesions. They show thick enhancing walls and intervening septae with multiple areas of mural defects communicating those adnexal lesions with the peritoneal cavity.
Splenomegaly is noted.
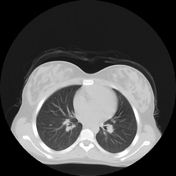
Scanned CT chest, revealed bilateral lower lobar thick atelectatic bands, likely representing pulmonary scarring of an old inflammatory process. No active inflammatory process or active TB.



Case Discussion
In this case with diffuse nodular peritoneal thickening and enhancement, and bilateral ovarian complex cystic lesions; The initial impression was carcinomatosis. However multiple signs were suggestive of tuberculous peritonitis including the following:
the young age of the patient and living in an endemic area of TB
the vaginal purulent discharge
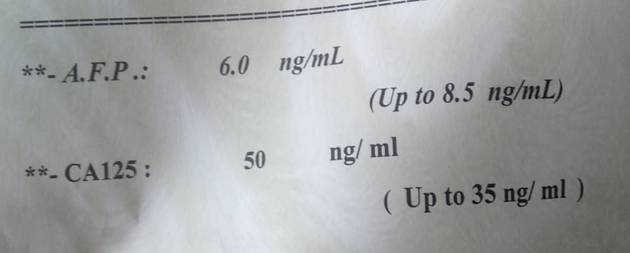
CBC analysis which revealed unexplainable anemia
radiological findings including enlarged necrotic right iliac mesenteric lymph nodes, mural thickening of the terminal ileum, splenomegaly, and the complex ovarian cystic lesions with enhancing defective walls
Ascites aspirate, surgical peritoneal biopsy and culture-confirmed tuberculosis (TB) resulting in tubo-ovarian abscesses (TOA).
Tuberculous peritonitis is misdiagnosed with peritoneal carcinomatosis and is an important differential diagnosis to keep in mind. Fluid aspiration, biopsy and culture are recommended to differentiate between those possibilities.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.