
Presentation
Abdominal pain and vomiting.
Patient Data






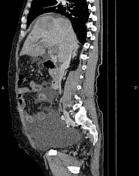
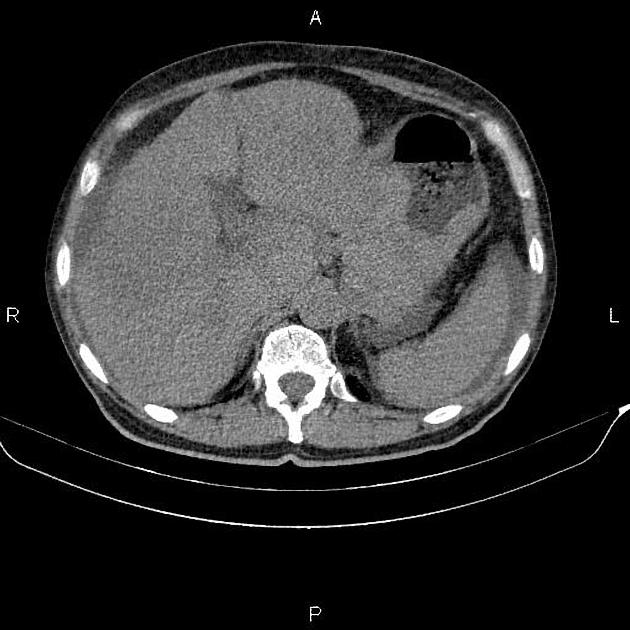
Marked increased wall thickness due to tumoral infiltration is present at gastric cardia and body. Multiple perigastric lymphadenopathies are seen with maximum SAD of 35mm. Local invasion is present to left liver lobe. Additionally, multiple low enhancing masses are seen at liver less than 85mm. Portal vein is completely thrombosed. Moderate ascites is present and there are several peritoneal soft tissue density masses less than 25mm inferring tumoral deposits.
Pancreatic duct is dilated.
The prostate gland is enlarged.
Degenerative changes as osteophytosis are seen at the lumbar spine.
Case Discussion
Pathology proven metastatic gastric adenocarcinoma. CT is currently the staging modality of choice because it can help identify the primary tumor, assess for the local spread, and detect nodal involvement and distant metastases.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.