
Presentation
Young adult, neutropenic bone marrow transplant patient, with a fever.
Patient Data



Chest x-ray demonstrates a Hickman line in situ. In the left mid-zone a region of ill-defined opacity is noted, seen anterior to the oblique fissure on lateral projection, thus within the left upper lobe. The pleural spaces are clear. A radio-opaque metallic structure is external to the patient, not seen on lateral view.
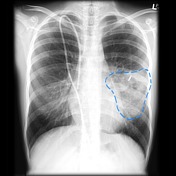
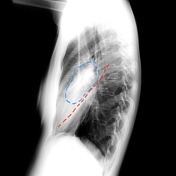
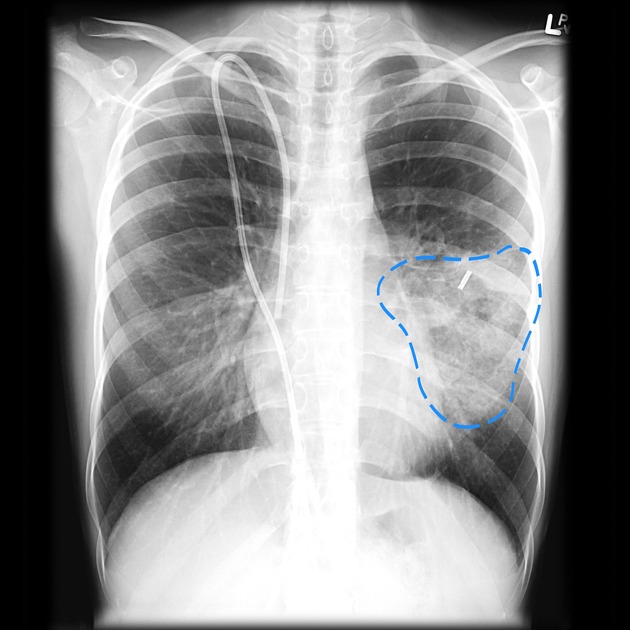
In the left mid-zone a region of ill-defined opacity is noted (blue dotted line), seen anterior to the oblique fissure (red dotted line) on lateral projection, thus within the left upper lobe.



Films obtained only four days earlier the lungs and pleural spaces are normal. This essentially excludes malignancy and any chronic process as the cause.
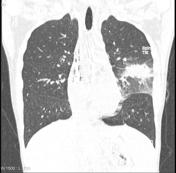



CT chest confirms consolidation of anterior aspect of the left upper lobe, surrounded by a halo of ground glass opacity. No cavitation.
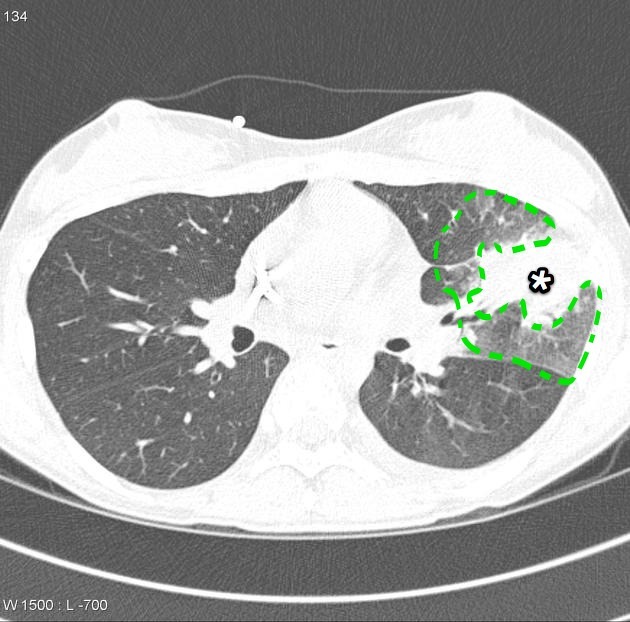
Solid region of consolidation ( * ) surrounded by a halo of ground glass opacity (green dotted line).
The patient was treated with amphoteracin B, and clinically improved. Follow-up imaging was obtained.



Chest x-rays obtained 10 days later demonstrate significant reduction in the size of the left upper lobe opacity.
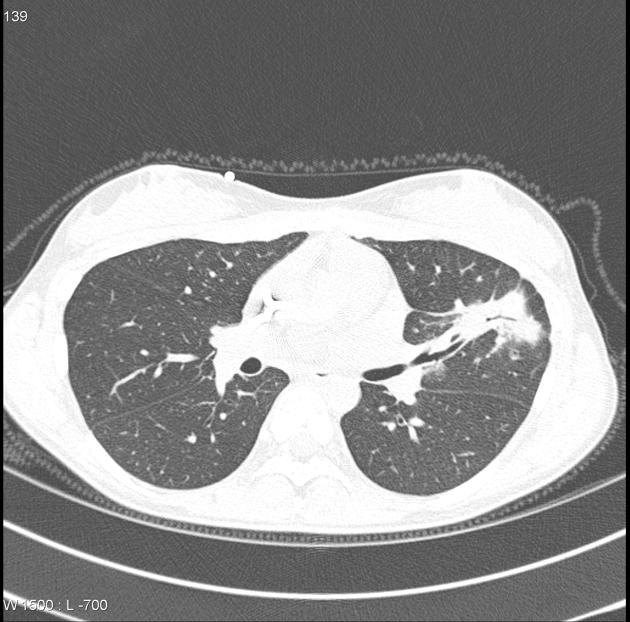
CT scan three weeks later still (one month after presentation) demonstrates a residual but much smaller nodular region of opacification with only minimal ground glass opacity.
Case Discussion
In a patient who is immunocompromised, there needs to be a low threshold for investigating for the possibility of angioinvasive aspergillosis, as without prompt treatment the infection can quickly overwhelm the patient.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.