
Presentation
Abdominal pain and diarrhea.
Patient Data
Age: 45 years
Gender: Male
From the case:
Active crohn disease




Download
Info
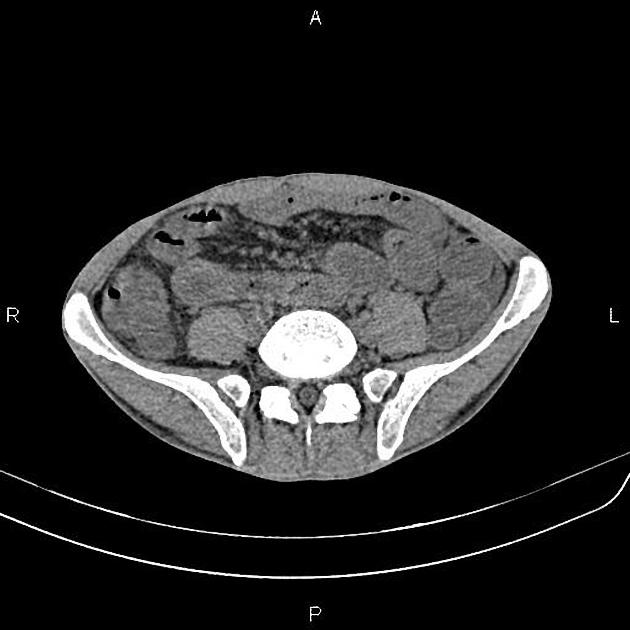
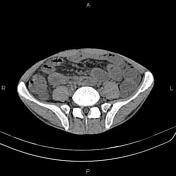
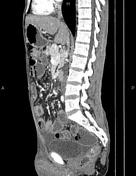
Circumferential increased wall thickness with skip areas is present at small bowel loops which shows mucosal hyper enhancement and accompanied by engorgement of the adjacent mesenteric vessels & mild fat stranding inferring Comb sign.
No frank fistulous formation is noted in current study. Several enlarged mesenteric lymph nodes are also evident in small bowel mesentery root. Mild to moderate free fluid is observed at abdominopelvic spaces.
Case Discussion
Features on CT scan are compatible with active Crohn disease.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.