
Presentation
Abdominal pain and dyspepsia.
Patient Data






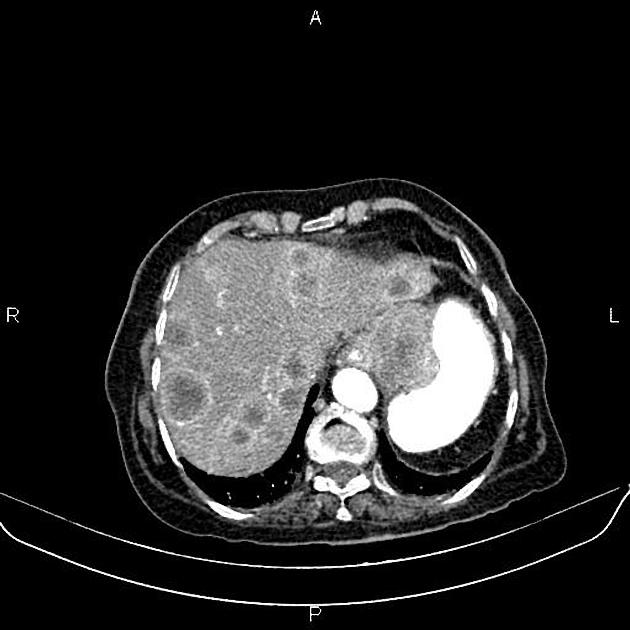
Marked increased wall thickness due to tumoral infiltration is present at the gastric cardia, subcardia, and proximal of the body, accompanied by perigastric fat stranding and a few regional lymphadenopathies with SAD less than 16 mm.
Multiple low enhancing masses are seen at the liver less than 45 mm.
Several gallstones are evident.
In imaged portions of the lower thorax, lymphadenopathy with SAD of 24 mm is noted at subcarinal regions.
There are also a few nodules less than 10 mm at visualized segments of both lung bases.
Degenerative changes as osteophytosis are seen at the lumbar spine.
Grade I spondylolisthesis of L5 on S1 is present with bilateral spondylolysis. Bilateral spondylolysis is also observed at the L4 level.
Case Discussion
Gastric mass; pathology proved adenocarcinoma, with regional and mediastinal lymphadenopathies, hepatic and pulmonary metastases.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.