
Presentation
Abdominal pain and dyspepsia.
Patient Data


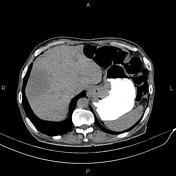

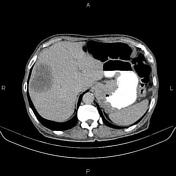


Increased wall thickness due to tumoral infiltration is present at gastric cardia, subcardia and proximal lesser curvature.
Lymphadenopathy with a SAD less than 16 mm are noted in the vicinity of the diseased segment. Lymphadenopathyy with SAD less than 15 mm are also observed at the porta hepatis and peripancreatic regions.
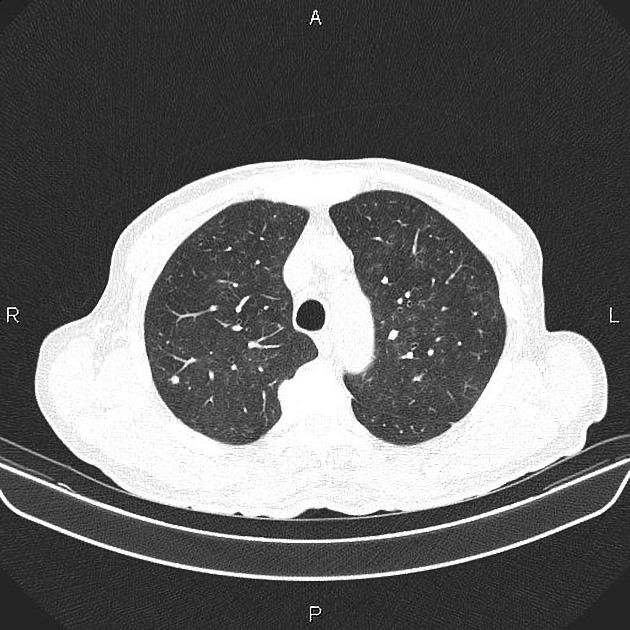
Several subpleural nodules are seen at both lungs less than 10 mm.
Additionally, a 70 mm low enhancing mass is seen at the right liver lobe which shows peripheral enhancement on delayed images.
The prostate gland is enlarged.
Case Discussion
Gastric mass; pathology proven adenocarcinoma with perigastric, portahepatis and peripancreatic lymphadenopathies, hepatic and pulmonary metastasis.
CT is currently the staging modality of choice because it can help identify the primary tumor, assess for the local spread, and detect nodal involvement and distant metastases.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.