
Presentation
Work up for abdominal pain and dyspepsia. Palpable epigastric mass on physical exam.
Patient Data







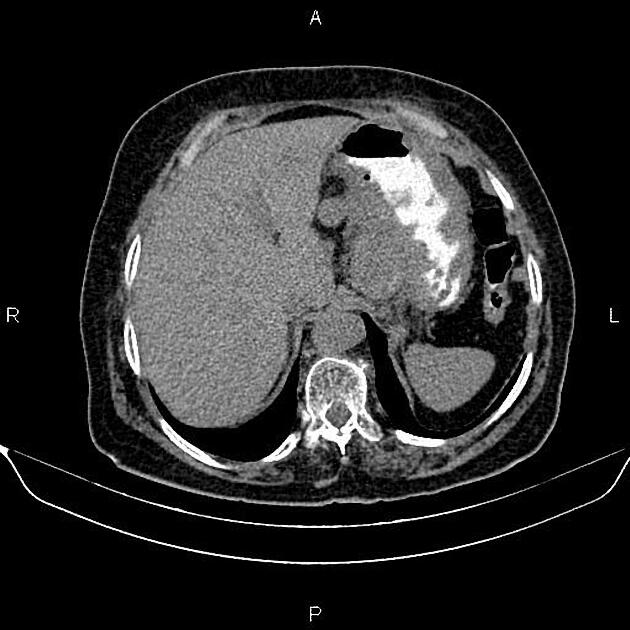
Increased wall thickness due to tumoral infiltration is present at the gastric cardia, subcardia and proximal of lesser curvature, accompanied by perigastric fat stranding.
Multiple enlarged lymph nodes are seen at perigastric, paraceliac and upper para aortocaval regions with SAD less than 45 mm.
A few subcentimeter simple cortical cysts are seen in the kidneys.
Degenerative changes such as osteophytosis are seen in the lumbar spine.
Anterior wedge fracture is present at the T12 vertebral body.
Grade I spondylolisthesis of L5 on S1 is also present.
Case Discussion
Pathology-proven gastric adenocarcinoma with perigastric, paraceliac and para-aortocaval lymphadenopathy.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.