
Presentation
Acute flair of ulcerative colitis. PR bleeding and syncope.
Patient Data




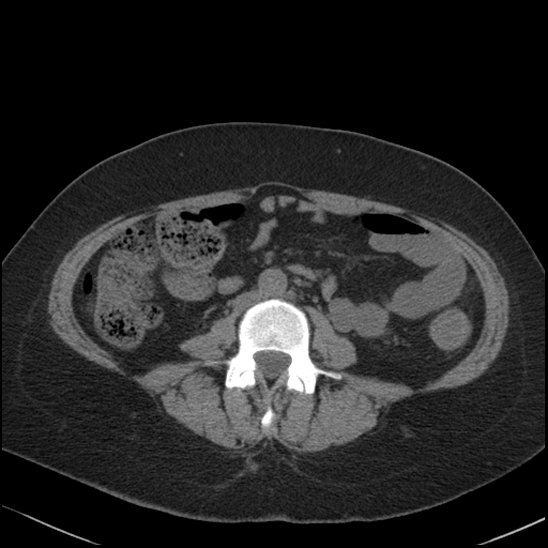
Intraluminal contrast extravasation is seen in the mid to distal third of the transverse colon, with increased pooling of contrast within the distal transverse colon and splenic flexure in the portal venous phase images. Mild circumferential mural thickening and edema of the mid transverse colon extending to the distal descending colon. No significant mesenteric fat stranding. The fluid-filled sigmoid colon and rectum is mildly distended containing mixed density material, likely representing altered blood. Multiple hyperdense discoid material within the rectum, cecum and stomach likely relating to medication tablets. The remaining large and small bowel are otherwise unremarkable .
No intra-abdominal free fluid or pneumoperitoneum. Normal vascular opacification of the major branches of the intra-abdominal vessels.
The liver, gallbladder, pancreas, spleen, adrenal glands and kidneys are normal. Intrauterine device in situ. Right ovarian cyst. No lymphadenopathy.
Imaged lung bases are clear. Moderate discovertebral degenerative change of the L5-S1. Right femoral head avascular necrosis.
IMPRESSION
Active arterial intraluminal hemorrhage within the distal third of the inflamed transverse colon.
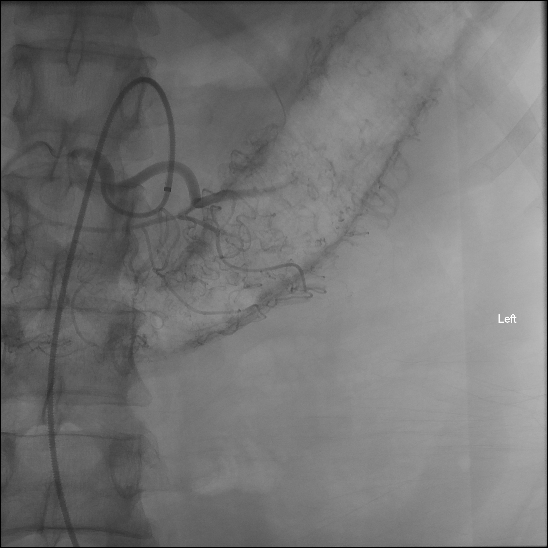
No bleeding source identified.
Case Discussion
The patient recovered uneventfully without a recurrent bleed. The right femoral head AVN is longstanding, due to longterm steroid use.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.