
Breast wound infection with chest wall sepsis and multifocal emphysematous osteomyelitis
Presentation
Had a right mastectomy for breast cancer five years ago. Reoperated for recurrence (partial resection) two months ago, presented with an infected wound, and dyspnea. CT angiography to rule out a pulmonary embolism.
Patient Data
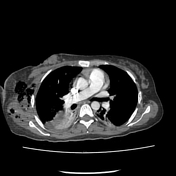

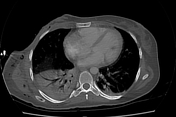

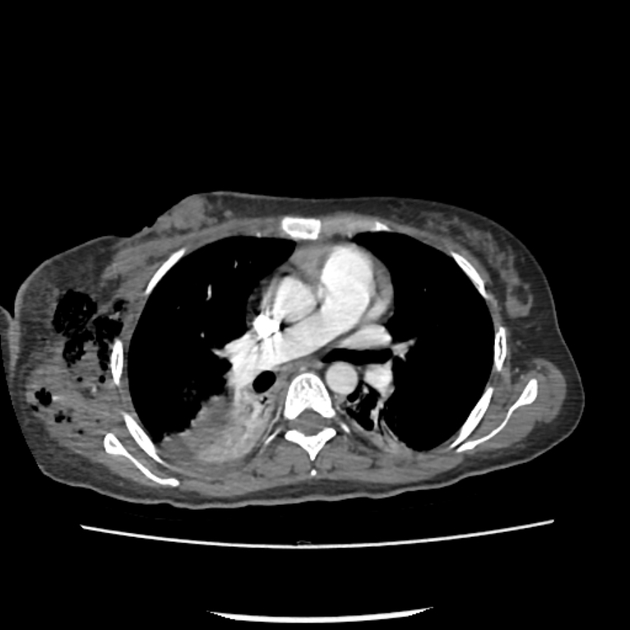
There is a soft tissue mass with irregular contours at the surgical scar, containing air bubbles, infiltrating the adjacent pectoral muscle with associated soft tissue gas collections of the right axillary region, chest wall, extending to the glenohumeral joint as well as within the right humeral head and scapula.
There is an intraosseous extension of gas collections into the vertebral bodies, clavicles, sternum, ribs, and prevertebral soft tissue, indicating multifocal osteomyelitis. Ill-defined osteolytic areas are seen within the vertebral bodies and sternum (metastases).
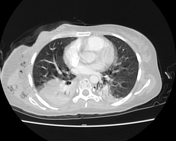
The lung window shows consolidation with air-bronchogram mainly of the dorsal segment of the upper lobe and lower lobe on the right and the dorsal segment of the upper lobe, and apical segment of the lower lobe on the left (pneumonia).
A small nodule (1.5 cm) is noted within the lower inner quadrant of the left breast (2nd primary vs metastasis).
Normal opacification of the pulmonary trunk, pulmonary arteries and their branches with no signs of pulmonary embolism.
Case Discussion
CT appearances of an infected breast wound with an underlying soft mass (remnant), extension of the infectious process to the chest wall with associated multifocal emphysematous osteomyelitis, pneumonia and bone metastases.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.