
Presentation
Chest pain with dyspnea.
Patient Data


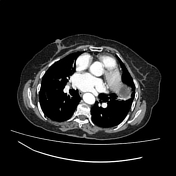



There is a large well-encapsulated mass (12 x 11 x 7 cm) within the myocardium of the left ventricle with no ehnancement seen following IV contrast, composed of multiple peripheral daughter cysts with central solid stroma. It appears in contact with the oesogastric junction as well as the aortic wall. Two other cystic lesions are seen, anterior to the previous mass, most likely of myocardial location, one unilocular of triangular shape (8x 4 x4 cm) and the other one partially calcified (2.4 x 2 x1.8 cm). There are small similar cysts seen at the right hilum and pericardium adjacent to the right atrium.
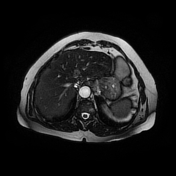
A calcified cyst (CE 5, according to the WHO classification) is noted in the segment IVa of the liver

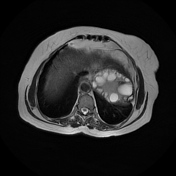
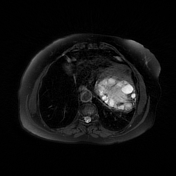
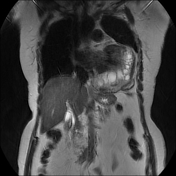
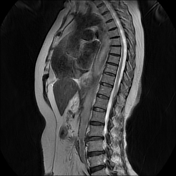
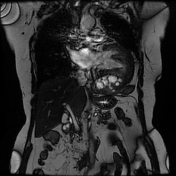
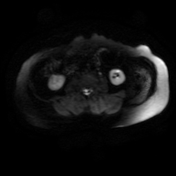
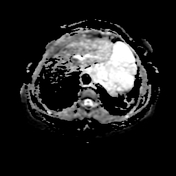
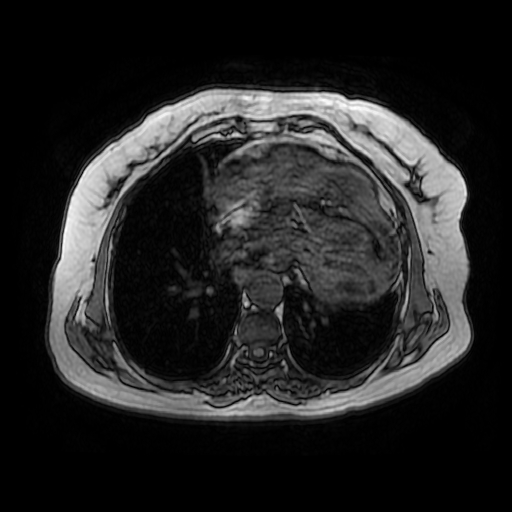
The main mass appears of myocardial location with peripheral low T1WI, high T2WI daughter cysts and a central solid stroma isointense to the myocardium on T1WI and slightly hyperintense on T2WI. The pericyst appears as a hypointense peripheral ring on T2 WI. The two other cysts are most likely of pericardial location. The small right myocardial cyst, as well as that of the right hilum, are better seen on CT than MRI.
The hydatid cyst of the liver is well-visualized with a hypointense calcified wall.
Case Discussion
Cardiac involvement in hydatid disease is uncommon, and account about 0.5 to 2% of hydatidosis. The left ventricle is the most common location (about 60%) and the pericardium about 10% of cases. The symptoms are variable directly related to the size and location of the cysts.
Both CT and MRI are helpful to precise the morphological features of the cysts as well as their location. CT is the best modality in the detection of the wall calcification, whereas MRI depicts better the anatomical location as well as the internal and external components of the cysts. Surgery is the treatment of choice
Additional contributors: R. Bouguelaa MD & A. Ghassiri MD.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.