
Presentation
Antenatal ultrasound at approximately 26 weeks gestation identified a left flank mass. Fetal MRI for reassessment.
Patient Data
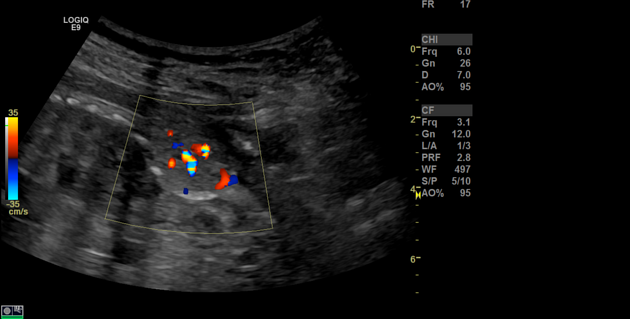
Limited sonographic images demonstrate a focal, elliptiform, solid-appearing, mildly echogenic, left flank mass, with increased vascularity. The lesion appears encapsulated with ill definition superiorly and is inseparable from the lateral abdominal wall muscles.

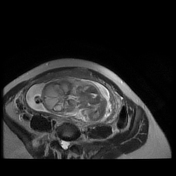
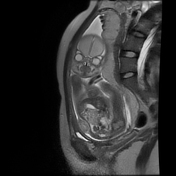
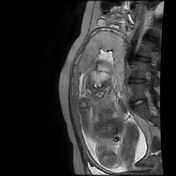
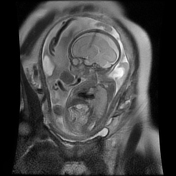
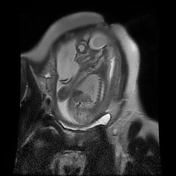
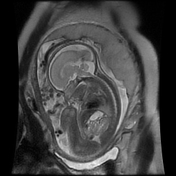
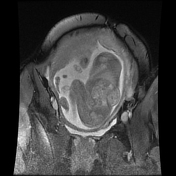
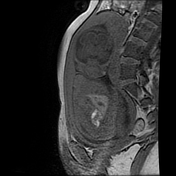
There is a single intrauterine gestation. The lie is vertex, with body part presentation (feet /buttocks). The occiput is left-sided and anterior. The placenta is fundal, posterior, and left-greater than right-sided. The liquor volume is satisfactory. The cervix is long and closed. Fetal motion and cardiac motion are evident.
Abdomen: There is abdominal situs solitus. The stomach is seen and is normal. The liver and gallbladder are normal. The cord insertion is normal. There is a 3-vessel cord. The right kidney is identified and appears normal. The bladder is filled and normal, with no extrophy.
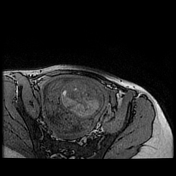
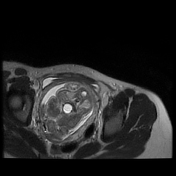
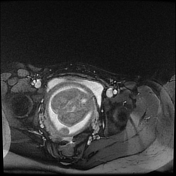
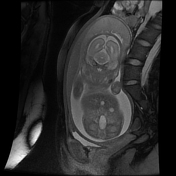
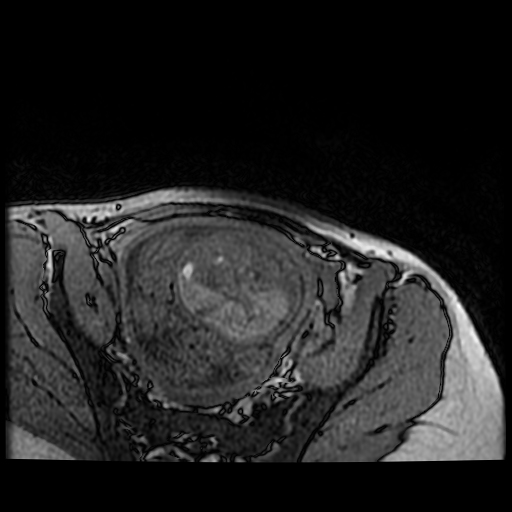
Consistent with the most recent ultrasound, a superficial left flank mass measuring 2.3 x 1.16 x 1.97 cm (CC X AP X W) was again seen. There is an apparent lateral abdominal wall defect measuring 1.08 cm in craniocaudal length. The regional left kidney is present and normal. The mass has a mixed signal intensity apperance with evidence of fluid/cystic components additionally. There are intra-lesional flow voids present. The mass has an elliptiform extra abdominal shape. There is a concave appearance of the left lateral flank wall due to extra-abdominal mass effect.
The rest of the fetal and maternal MRI assessment is normal.
Case Discussion
A histopathologically confirmed case of a left flank, intramuscular hemangioma. The lesion was completely excised a few days after birth.
The broad differential diagnosis included a rhabdomyosarcoma, possible renal (nephroblastoma), or adrenal (neuroblastoma) due to proximity to the left kidney and left adrenal gland. A lymphatic malformation could be considered as well.
There was no sonographic or MRI evidence to confirm a lateral abdominal wall hernia, given a possible abdominal wall defect on MRI assessment.
The presence of intra-lesional vascularity on ultrasound and the presence of flow voids including muscular epicenter alludes to the confirmed diagnosis of a congenital intramuscular hemangioma, which was successfully excised without any post-operative complications.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.