
Presentation
Acute onset confusional state with past history of fever, cough and abdominal pain.
Patient Data

Scattered bilateral reticular and nodular shadows more evident at the right middle and lower zone.
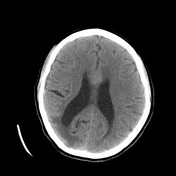

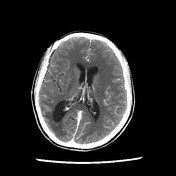
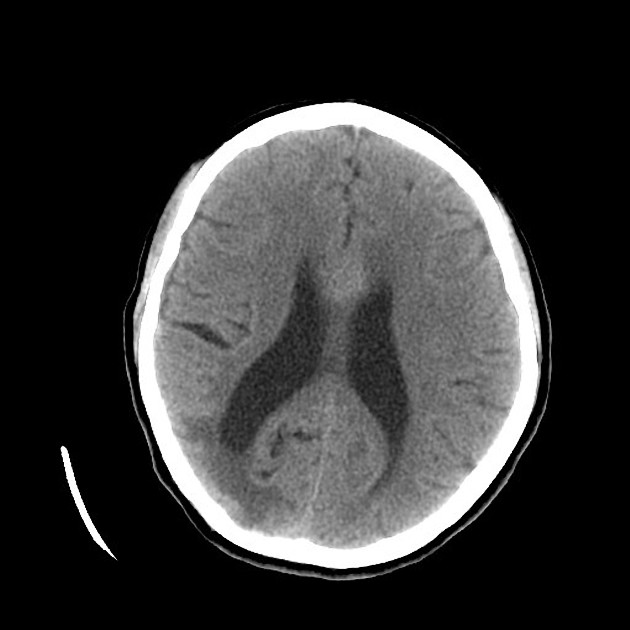
Pre and post contrast CT of the brain showing right occipital and bilateral parietal cortical and subcortical hypodensity with subtle nodular heterogeneous enhancement in the right occipital region as well a linear ring-like enhancement see in the para-midline parietal regions bilaterally.

TB meningitis with ring-enhancing parenchymal lesions (tuberculomas).
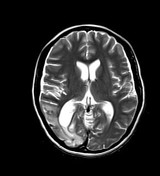
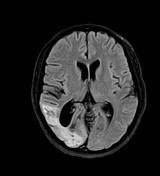
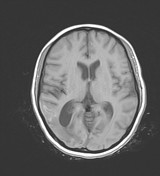
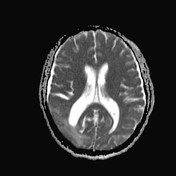
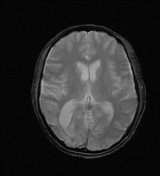
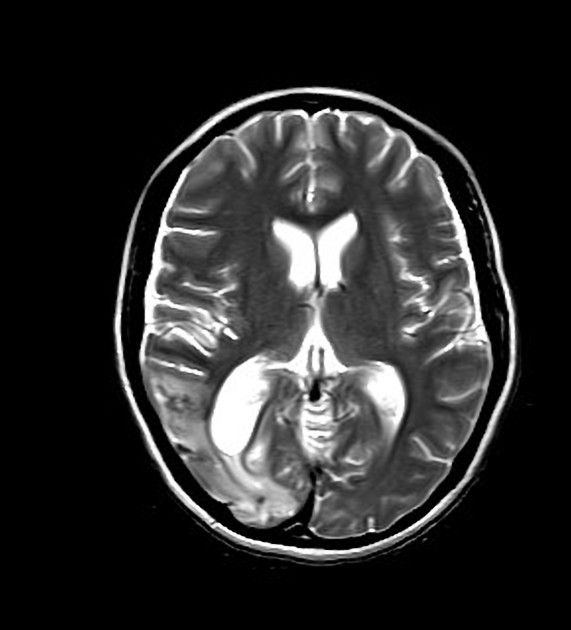
Multiple focal T2 and FLAIR hypointense lesions in the right occipital, bilateral parietal para-sagittal and bilateral cerebellar regions with related variable degrees of vasogenic edema. The related vasogenic edema can be clearly demonstrated after CSF signal is attenuated. The lesions are iso to hypointense on T1. The related edema reflects hypointense signal. However, there is linear meningeal and gyriform T1 hyperintense signal in the right occipital region as well as scattered heterogeneous hyperintensities at the para-sagittal parietal regions.
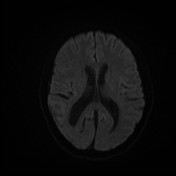
Increased ADC values, confirming no diffusion restriction.
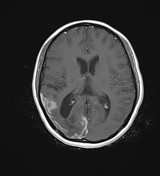
Intense post contrast peripheral ring enhancement of the previously described lesions (tuberculomas) together with evident thickened enhancing meninges at the right occipital cortex, right tentorial leaflet and posterior aspect of the falx. Multiple signal void areas are appreciated coinciding with the hyperintensities demonstrated on non-enhanced T1, confirming the hemorrhagic nature of this signal. Meningeal involvement is clearly demonstrated. Some of the lesions (tuberculomas) are also seen to be dural-based. Involvement of the corpus callosum is also noted.






Post-primary TB of the lungs. TB granulomas at the liver, spleen and kidneys. TB of the spine involving T5, S1 and S2 vertebral bodies with prevertebral and bilateral psoas abscesses.
Left apical cavitary lesion with scattered coarse reticulonodular densities, fibrotic changes and few small ill-defined patches of consolidation. Changes are appreciated at the upper lung zones. No significant hilar or mediastinal lymphadenopathy.
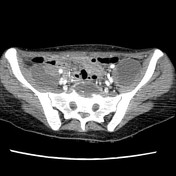
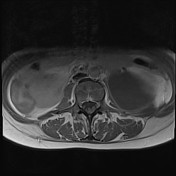
Scattered small rounded well-defined hypodensities seen in the liver, spleen and both kidneys, suggesting TB granulomas. There are also bilateral fluid densities at the iliopsoas muscles more on the left side showing average wall enhancement, in keeping with iliopsoas abscesses. Prevertebral and presacral fluid attenuation with enhancing walls at L5, S1 and S2 levels with extension to L5-S1 disc.
Axial scans of the pelvis demonstrating the extent of the prevertebral and presacral abscess together with the bilateral iliopsoas abscesses, the left side is larger in size, however, there is evidence of multiple loculi on the right side.
Lytic and sclerotic changes at L5 and S1 vertebral bodies with irregularity and destruction seen at L5-S1 disc.
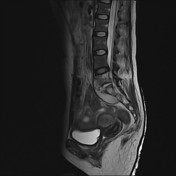

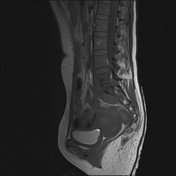
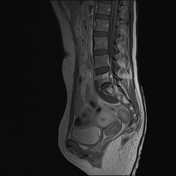
Pott disease of the lumbosacral spine with bilateral iliopsoas abscesses.
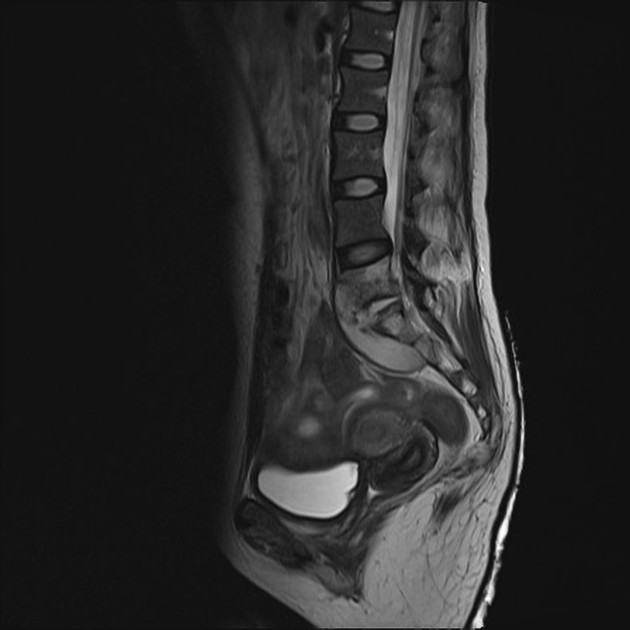
Paraspinal collection anterior to L5 and S1 vertebral bodies with subligamentous spread (beneath the anterior longitudinal ligament) and extension to the L5-S1 disc which narrowed and showing disrupted endplates. There is also evident marrow edema at the affected vertebrae. Postcontrast marginal enhancement of the paraspinal fluid collection together with marrow enhancement of the affected vertebral bodies. No definite enhancement is seen in the affected disc space.
Case Discussion
Miliary tuberculosis is a widespread form of the disease as a result of hematogenous spread of Mycobacterium tuberculosis. It is classically referred to miliary pulmonary tuberculosis which usually appears as miliary pulmonary nodules and pleural effusion on chest radiographs and on CT scans. There can be associated or isolated Extrapulmonary Tuberculosis as a result of this hematogenous spread of the disease, classically appearing widespread TB granulomas of the affected organ/organs. However certain forms of the disease exist manifesting with specific findings such as TB affection of the CNS (TB meningitis and TB meningoencephalitis) and tuberculous spondylitis (Pott Disease).
It is more common to occur in individuals of lower socioeconomic status. In many cases, such as the one in hand, the presentations of pulmonary TB can be subtle and nonspecific and the patient can present later by extrapulmonary affection which can happen in a wide range of organs. However pulmonary TB is usually present in the post-primary form, which can present in variable forms depending on the severity ranging from scattered reticulonodular opacities, cavitary lesion or widespread miliary TB nodules and pleural disease.
TB granulomas can affect many organs including the brain, where it present as ring-enhancing parenchymal lesions that have to be differentiated from other ring-enhancing lesions, however the presence of meningeal involvement narrows the differential diagnosis. TB granulomas can also affect, as in our case, variable abdominal organs such as the liver, spleen and kidneys, and can result in variable degrees of organ dysfunction depending on the severity of the disease.
Osseous involvement is another consequence of hematogenous spread of tuberculosis, in addition there may be spinal disease or TB spondylodiscitis resulting in abscess formation and the classical Pott disease. Cross-sectional imaging can clearly show the extent of the affected vertebrae and the related paraspinal or epidural fluid collection.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.