
Presentation
History of thoracic aortic aneurysm on surveillance. Presenting with new AF.
Patient Data



Cardiomediastinal contour is normal. When compared to prior imaging (not shown), persistent blunting of the right costophrenic recess is in keeping with longstanding pleural thickening. Ill-defined opacities in the right mid to lower zone with known round atelectasis. No evidence of acute pulmonary edema. The left pleural space is clear.
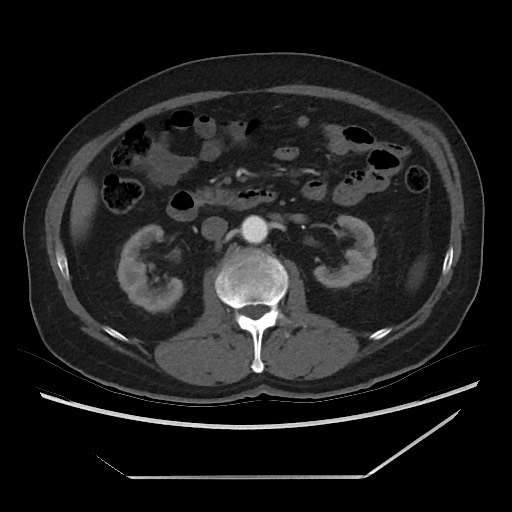
Partially calcified outpouching of the distal aortic arch measuring approximately 4.4 cm in maximal diameter - most probably a ductus diverticulum or an old post-traumatic aortic pseudoaneurysm. Unchanged in size, shape, and appearance compared to the study from 2 years prior (not shown). The remainder of the aorta is unchanged as well.
Round atelectasis within the right lower lobe, appears slightly larger than the previous study.
There is apparent soft tissue density arising from the right lower lobe pleura that has increased in size, measuring approximately 3.2 x 4.7 cm (approximately 2.6 x 1.7 cm on the previous CT scan). This is suspicious for a pleural-based mass and consideration for a biopsy is recommended.
The remainder of the lungs is clear. Small right-sided pleural effusion.
New suspicious subcarinal lymph node. New 1.8 cm retrocaval soft tissue mass, suspicious for lymphadenopathy.
The abdominal viscera are unchanged. The adrenal glands are unremarkable. No other lymphadenopathy.
Conclusion:
Unchanged ductus diverticulum vs. old aortic pseudoaneurysm.
Increase in size of a soft tissue mass arising from the right lower lobe pleura.
New subcarinal and retrocaval lymphadenopathy.
Consideration for a pulmonology opinion +/- biopsy is recommended.



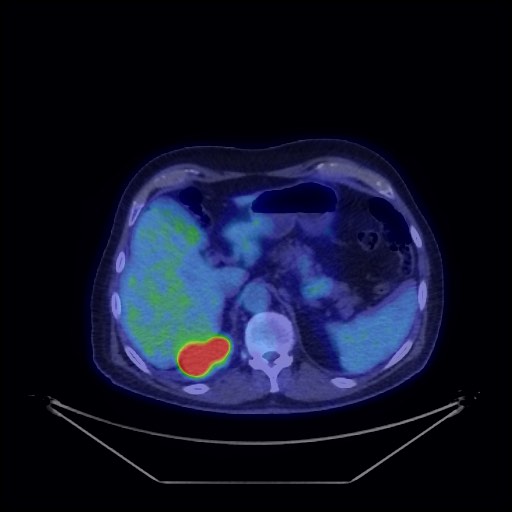
There is intense FDG uptake in the lobulated pleural-based mass located in the basal right lung, which measures 66 x 36 x 61 mm. This abuts the posteromedial pleura and deforms the diaphragm. No definite diaphragmatic invasion is apparent; however, assessment is limited on low-dose CT. A non-FDG avid density located immediately cranial to the pleural lesion most likely reflects adjacent rounded atelectasis. There is a non-FDG avid thickening of the adjacent right pleura.
Focal mild FDG uptake is present in an adjacent 8 x 6 mm right lower lobe pulmonary nodule (best appreciated on respiratory-gated images), suggestive of a satellite lesion.
Intensely FDG avid subcarinal node (28 x 14 mm) and retrocaval node (22 x 30 mm) are consistent with metastatic disease. There is no concerning FDG avid lymphadenopathy elsewhere in the right hilar or mediastinal regions. Mild FDG uptake in a small AP window node is most likely reactive.
No FDG avid lesions are demonstrated elsewhere.
Elsewhere in the imaged body physiologic FDG activity is present.
Conclusion:
Intensely FDG avid right pleural-based malignancy, which abuts and deforms the right diaphragm. There is a small satellite lesion in the adjacent right lower lobe. Intensely FDG avid metastases involving a subcarinal and a retrocaval node. No evidence of distant bone or visceral metastases.

Under sonographic guidance, a 16 gauge core biopsy needle was inserted into the lesion and a single pass was performed. Good quality sample.
No immediate complications.
Samples were sent to pathology for analysis.
Case Discussion
This patient has a known background of previous asbestos exposure and longstanding calcified and soft tissue pleural plaques. He had previous imaging in the past showing chronic round atelectasis in the right lung base and was under surveillance at vascular surgery due to an aortic arch aneurysm.
CTA showed a pleural mass and thoracic and extra-thoracic lymphadenopathy. Given the location of the mass and previous exposure to asbestos, the possibility of mesothelioma was raised.
US-guided core biopsy was performed:
Macroscopy: Labeled "Right pleural lesion 16G core biopsy". Core biopsy 19 mm.
Microscopy: The biopsy core consists entirely of malignant tumor formed by partly necrotic sheets of atypical epithelioid cells. Tumor cells have moderately pleomorphic nuclei with prominent nucleoli and a moderate amount of eosinophilic cytoplasm. No glandular or papillary arrangements are seen and there is no keratinization.
Immunostains have been performed and the tumor cells have the following immune profile:
Positive: HBME1, CK5/6 (patchy), calretinin (weak and focal), CK7 (a small minority of cells only).
Negative: TTF1.
Additional immunostains have been performed and the tumor cells show strong positive staining for mesothelial markers EMA and WT1 and do not stain with the squamous marker p40. These findings support the original diagnosis of malignant mesothelioma.
Conclusion: Right pleural lesion, core biopsy: Epithelioid mesothelioma.
After MDM discussion (Stage IV T2 cN1 M1 (extra-thoracic lymph node), this patient was offered chemotherapy (Carboplatin/pemetrexed).


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.