
Round atelectasis, also known as rounded atelectasis, folded lung or Blesovsky syndrome, is an unusual type of lung atelectasis where there is infolding of a redundant pleura. The way the lung collapses can at times give a false mass-like appearance.
On this page:
Epidemiology
Associations
Round atelectasis may be associated with:
asbestos lung exposure 3: most commonly
therapeutic pneumothorax in the treatment of tuberculosis 1
post-infectious pleural inflammation / parapneumonic effusion
Pathology
Two theories have been put forward. The second theory is more favored while the multifactorial etiology suggests both mechanisms probably operate in different patients:
-
Hanke and Kretzschmar
underlying pleural effusion causes local atelectasis in the adjacent lung
a cleft or infolding of the visceral pleura will then form if the rate of pleural fluid formation exceeds alveolar air absorption
this then causes the lung to tilt on the cleft
the lung then curls on itself in a concentric fashion
fibrous adhesions suspending the atelectatic segment (and usually tilt the lung cranially) develop
as the effusion resorbs, the aerated lung fills in the space between the area of round atelectasis
organization of the fibrinous exudate and fibrous contraction lead to additional lung parenchymal distortion
-
Schneider et al. (expanded on by Dernevik and colleagues)
a local pleuritis caused by irritants such as asbestos
in the event of a benign asbestos-related pleural effusion, the pleura contracts and thickens with shrinkage of the underlying lung, and atelectasis develops in a round configuration
Etiology
exposure to mineral dust: asbestosis, pneumoconiosis 13
exudative pleuritis: tuberculosis, hemothorax 13
less commonly seen in histoplasmosis, legionella, end-stage renal disease 13
sarcoidosis 13
Location
There may be a predilection towards the lower lobes 4.
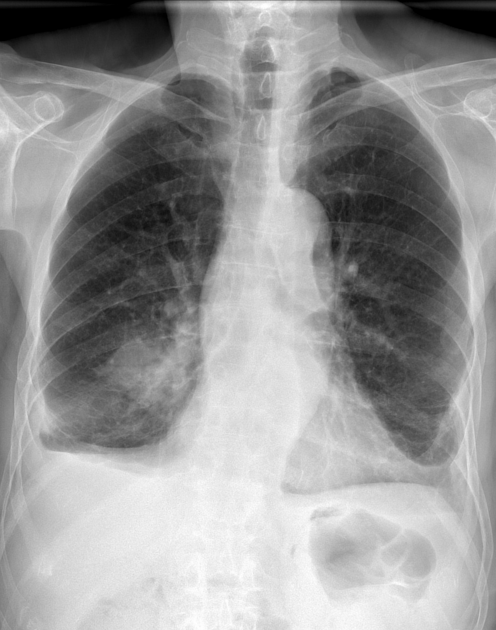
Radiographic features
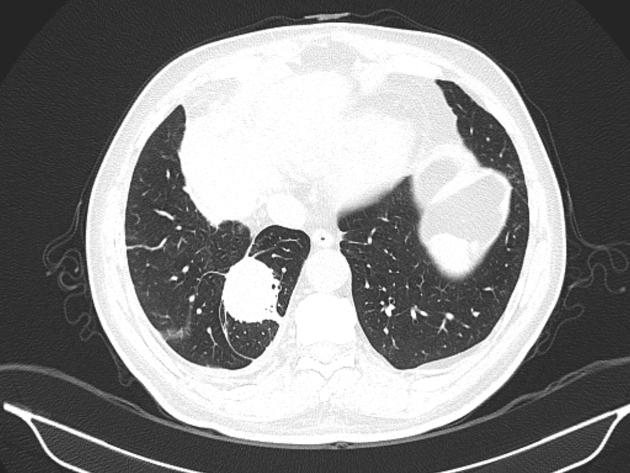
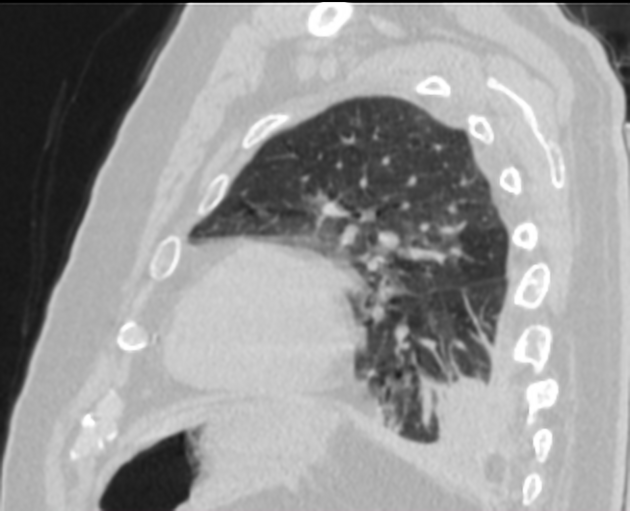
CT
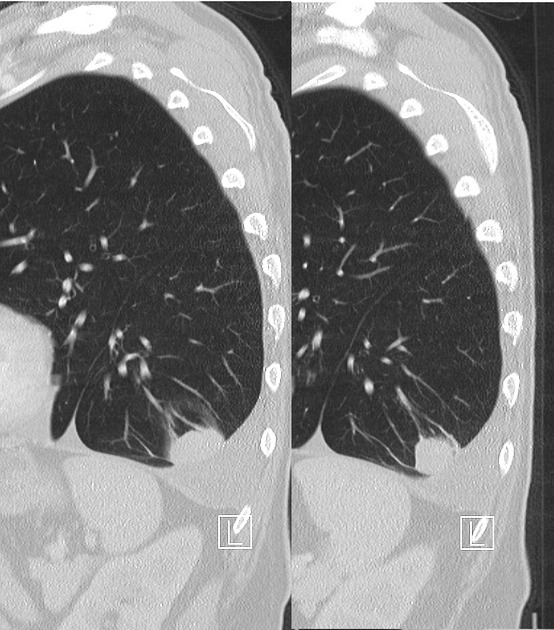
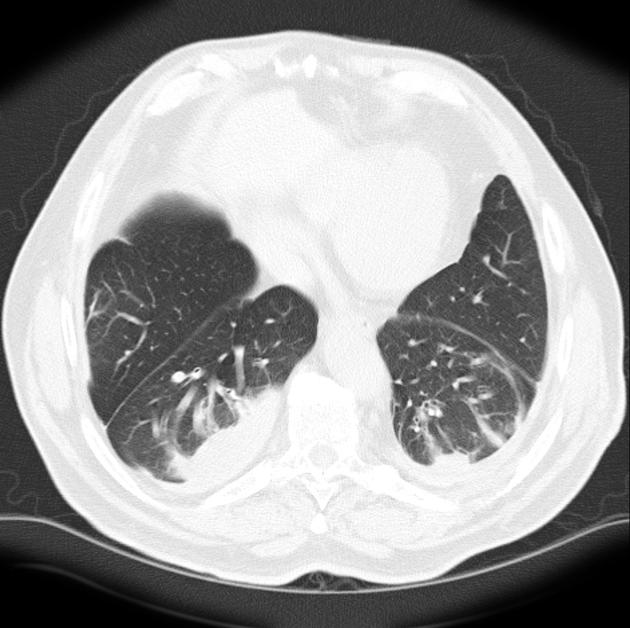
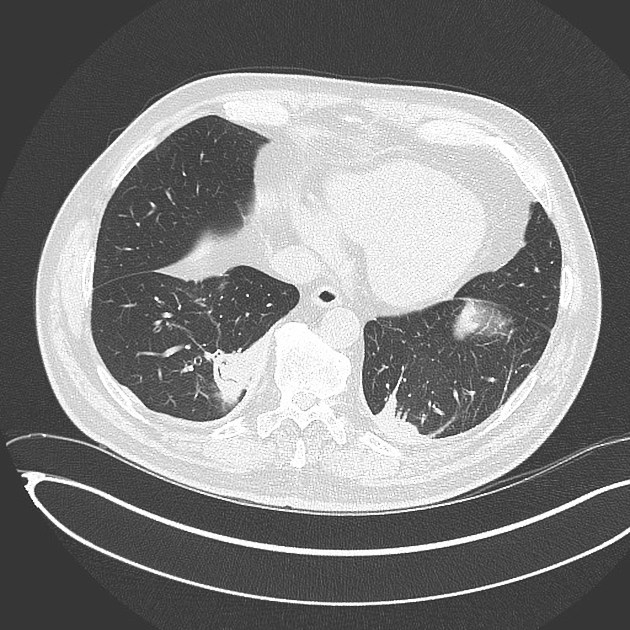
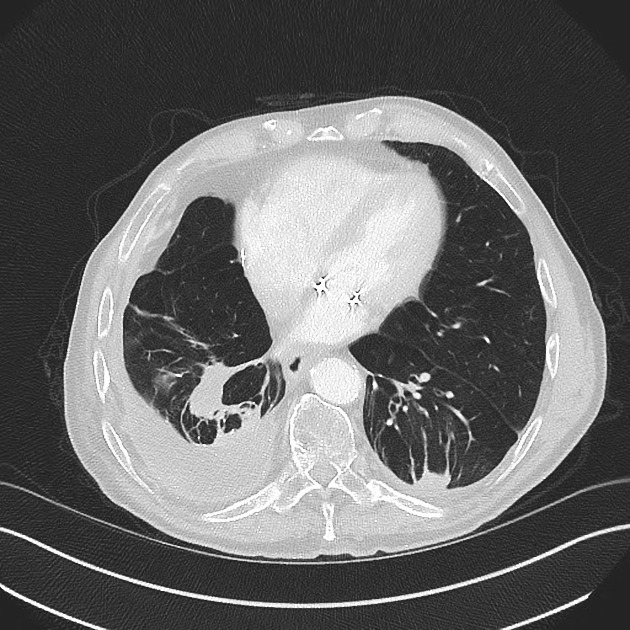
round or oval in shape
almost always seen adjacent to a pleural surface
there is associated adjacent pleural abnormality, e.g. pleural thickening or pleural effusion
comet tail sign 2: produced by the pulling of bronchovascular bundles giving the shape of a comet tail
as it represents collapsed lung, it commonly demonstrates a typical parenchymal enhancement
posterior lower lobes are most commonly involved and, sometimes, bilateral or symmetrical 14
Rounded atelectasis can occasionally increase in size on serial scans 6,7.
Nuclear medicine
FDG-PET
not metabolically active
may play a role in differentiating from malignancy when there are few or atypical features on chest radiographs and CT 9
Diagnosis
All five of the following findings must be present to diagnose round atelectasis:
1) Adjacent pleura must be abnormal.
2) Opacity must be peripheral and in contact with the pleura.
3) Opacity must be round or elliptical.
4) Volume loss must be present in the affected lobe.
5) Pulmonary vessels and bronchi leading into the opacity must be curved — this is the comet tail sign15.
History and etymology
It was first described by Loeschke in 1928 6.






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.