
Presentation
Abdominal pain, nausea and vomiting
Patient Data
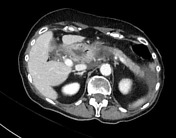


Motion degraded exam. Acute interstitial pancreatitis evidenced by unorganised, acute peripancreatic fluid/stranding with a mildly dilated main pancreatic duct. No areas of hypoenhancement to suggest a necrotizing component. Portal, splenic, superior mesenteric veins patent.
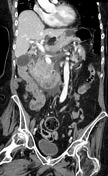
Cholelithiasis with several small stones within the cystic duct. Mild gallbladder wall thickening with pericholecystic fluid. Small gallstone within the distal common bile duct a few centimeters above the ampulla (this can be particularly well appreciated on coronal reconstructions).
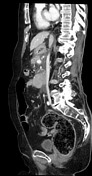
Lung findings were imaged separately. Massive amount of stool in the rectum with rectal wall thickening. No surrounding stranding or fluid.
Case Discussion
For this patient, the lipase was >1500 U/L (exceeds assay range of analyzer).
Combination of findings of cholelithiasis, stones in the cystic duct, choledocholithiasis, and acute interstitial pancreatitis. This makes the diagnosis of gallstone pancreatitis almost certain, although no definite stone is seen at the level of the ampulla.
The inflammation of the gallbladder is favored to be reactive in the setting of acute pancreatitis; however, given the stones in the cystic duct, superimposed acute cholecystitis would also be possible and correlation with laboratory and physical examination findings was recommended.
Also note massive amount of stool in the rectum with wall thickening, placing the patient at risk for stercoral colitis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.