
Presentation
Patient with 4 weeks of progressively worsening exertional dyspnea. History of uterine mass removed 5 years ago.
Patient Data
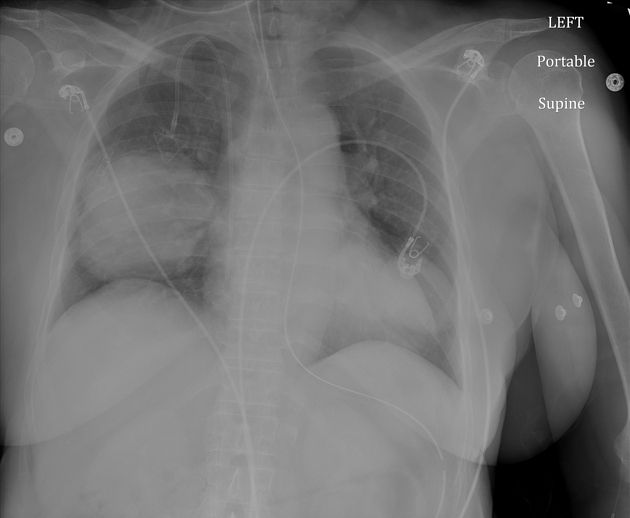
Chest radiograph shows bilateral lower lung masses. Endotracheal tube, enteric tube, and right internal jugular approach port catheter are noted.


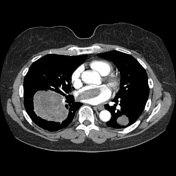
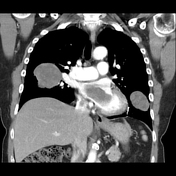

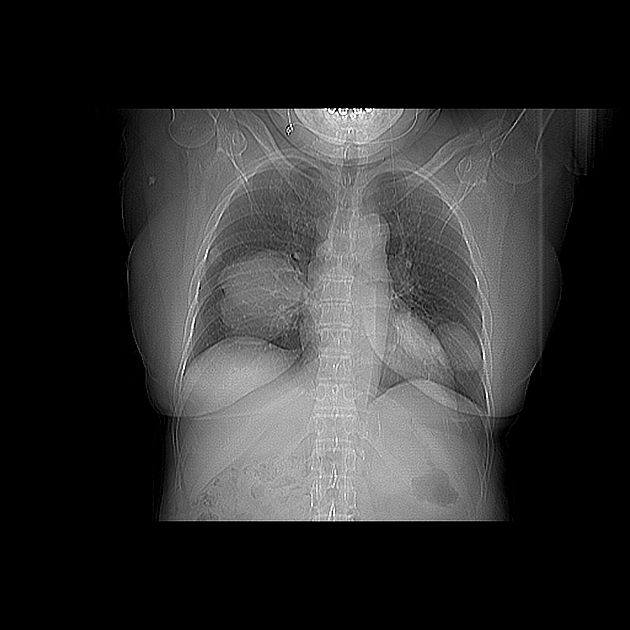
Large right lung mass invades right pulmonary vein, extending into the left atrium and abutting the mitral valve.
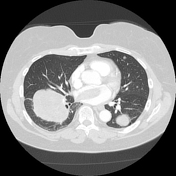
Multiple bilateral pulmonary nodules and masses, largest in the lower lobes.
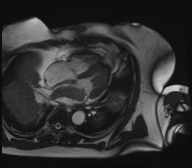
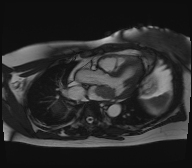

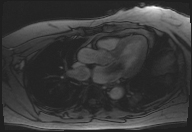
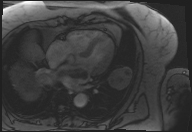
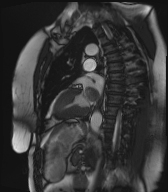
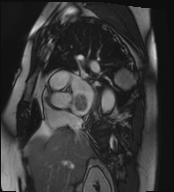
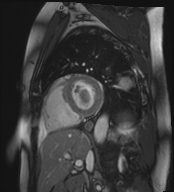
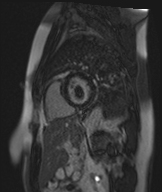
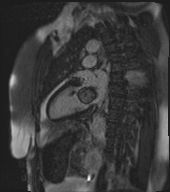
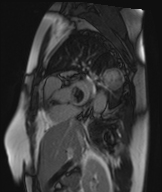
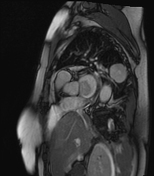
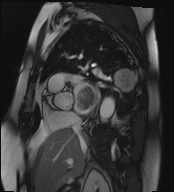
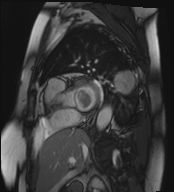
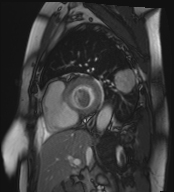
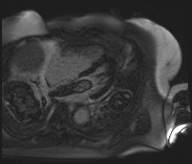
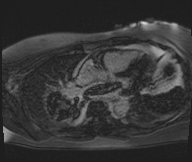
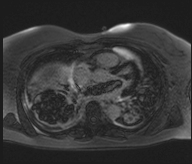
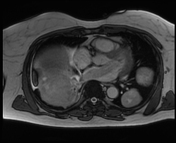
Multiple dynamic sequences demonstrating large right lung mass extending into the left atrium, extending transiently beyond the mitral valve into the base of the left ventricle. This highly mobile mass measures approximately 9 cm x 2 cm and shows enhancement on the post-contrast sequence.
Multiple enhancing bilateral pulmonary nodules and masses.
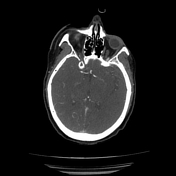
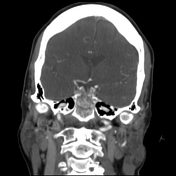
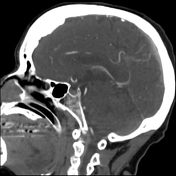

CT angiogram of the head and neck shows occlusion of the right middle cerebral artery and left middle cerebral artery in the M1 segments. There is also a large filling defect consistent with occlusion of the mid basilar artery.
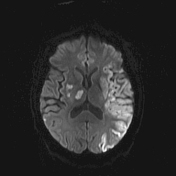
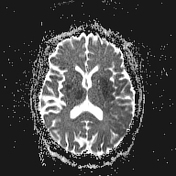
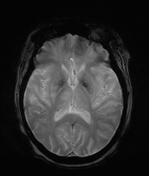
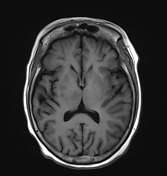
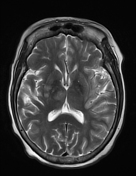
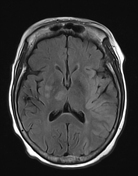
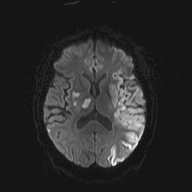
Large area of diffusion restriction in the left frontal, parietal, temporal, and insular cortices, consistent with watershed area of left middle cerebral artery.
Diffusion restriction in the right thalamus, corona radiata, and lentiform nucleus, consistent with occlusion of lateral lenticulostriate arteries.
Multiple punctate foci of diffusion restriction in the bilateral cerebellar hemispheres.
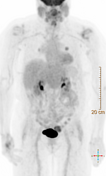
Left lower lobe subpleural pulmonary nodule with increased FDG uptake, SUV max of 5.7.
Right lower lobe perihilar pulmonary nodule with SUV max of 3.8.
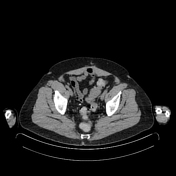
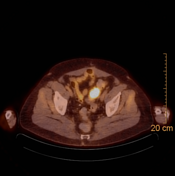
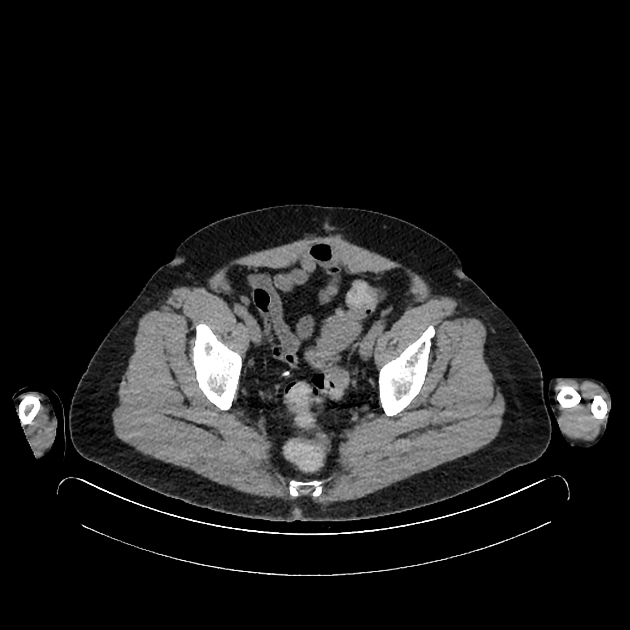
Sigmoid colon mass with increased FDG uptake, SUV max of 9.7.
The uterus is surgically absent.
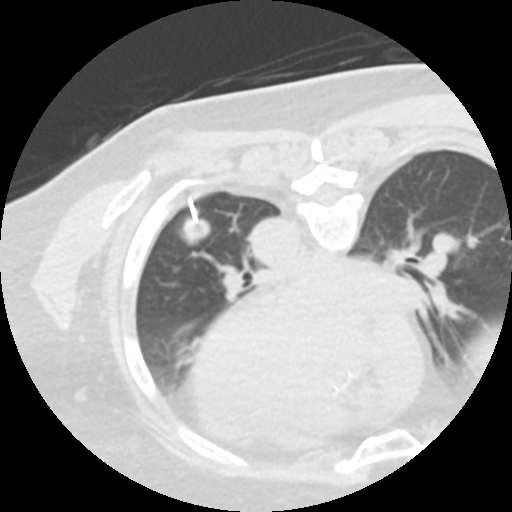
CT-guided core biopsy of pulmonary nodule in the left lower lobe from a posterior approach.





There is a large, partially calcified mass in the uterus, which is diffusely enlarged (11.5 cm x 10 cm x 10 cm). There is no significant pelvic adenopathy.
Case Discussion
Hospital Course:
This patient had a history of a rapidly enlarging, calcified pelvic mass and subsequently underwent total abdominal hysterectomy with right salpingo-oophorectomy about five years ago. Pathology was consistent with well-circumscribed, necrotic and degenerated leiomyoma with minimal atypia and no mitoses.
About two years ago, multiple new lung nodules were detected. Staging PET/CT also demonstrated a 5 cm sigmoid mass. Lung and sigmoid colon resections yielded tissue consistent with metastatic leiomyosarcoma.
Now, the patient presents with 4 weeks of exertional dyspnea. Pulmonary nodules were determined to be larger in size with presumed intra-cardiac tumor thrombus. During the hospital stay, the patient experienced a thromboembolic CVA and elected to enter hospice care.
----------------------------------------------------------------------------
Pathology - Lung Mass:
Specimen(s) Received - LEFT LOWER LOBE WEDGES #1 (0.8 cm); #2 (1.8 cm and 0.6 cm)
Lobar specimens demonstrate multiple well-demarcated sections of highly pleiomorphic spindle cells with high mitotic activity (20/10 HPF). Focal tumor necrosis is noted. Immunostains were diffusely positive for SMA, calponin, and desmin. Ki-67 and p53 immunostaining demonstrates labeling index greater than 60%. Pathological features are consistent with diagnosis of metastatic leiomyosarcoma.
Pathology - Sigmoid Colon Mass:
Specimen(s) Received: SIGMOID MASS (5.0 cm x 3.4 cm x 3.3 cm)
Highly pleiomorphic spindle cells with high mitotic activity and focal necrosis are observed. Immunostaining is diffusely positive for SMA and desmin and negative for calretinin and CD10. Findings are consistent with diagnosis of metastatic leiomyosarcoma.
Pathology - Uterine Mass (5 years prior):
Specimen(s) Received: FSA - UTERINE FUNDA + RIGHT ADNEXA
Specimen is well-circumscribed, nearly entirely necrotic with minimal foci of viable cells. Nuclei are largely bland in appearance, spindle-shaped with minimal atypia and no evidence of mitoses. Immunostaining for p53 is negative (wild-type). Features are consistent with leiomyoma with extensive necrosis and degeneration.
----------------------------------------------------------------------------
Discussion:
Uterine leiomyosarcomas (LMS) are rare, highly aggressive smooth-muscle neoplasms with a 5-year recurrence rate ranging from 45-75% and a 2-year survival rate of under 50% for metastatic disease 1. Pulmonary metastases are extremely common, with around 40% of first LMS recurrences identified in the lungs 1. While most cardiac metastases secondary to LMS involve the right heart due to hematogenous invasion of the IVC, direct extension of tumor into the pulmonary veins and into the left heart has been reported with large mediastinal tumors 2. Intracavitary tumor thrombus may result in valvular dysfunction, cardiac arrhythmias, and heart failure 3, consistent with this patient's 1-month left ventricular ejection fraction decrease from 60% to 30% with increased right atrial pressures. Management of cardiac metastases is most often surgical, but shared decision-making is vital especially for patients with advanced metastatic disease at multiple sites 4. While medical treatments provide short-term symptomatic relief, intracavitary masses may lead to thrombus formation or even tumor embolism 5, as is suspected in the case of this patient's bilateral MCA and basilar artery occlusions.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.