
Presentation
The patient has known idiopathic intracranial hypertension. There is a poor clinical response to inserting a lumboperitoneal shunt—a work-up for shunt malfunction.
Patient Data






Elevate BMI with left lateral wall laxity and features suggest a lateral ventral hernia.
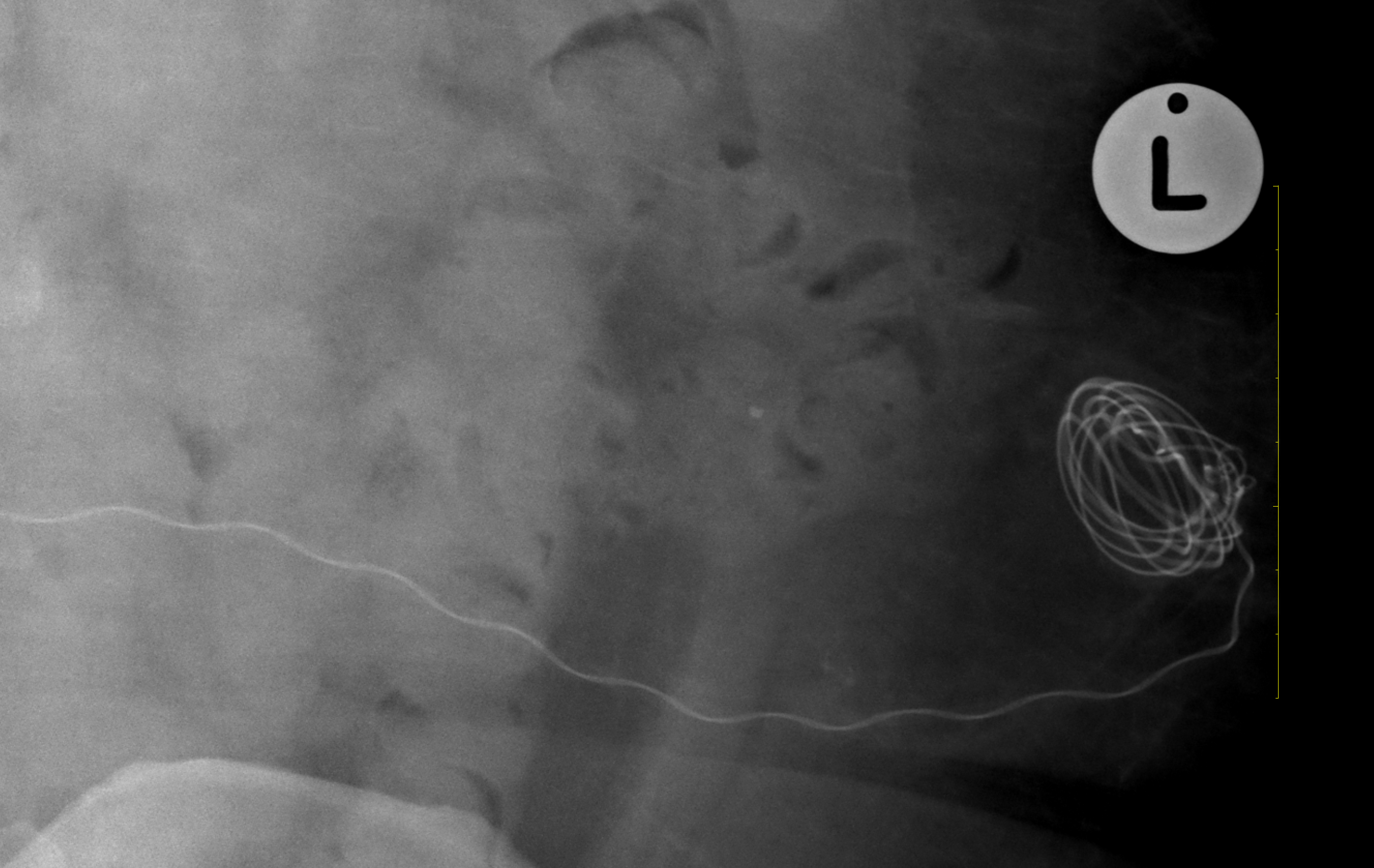
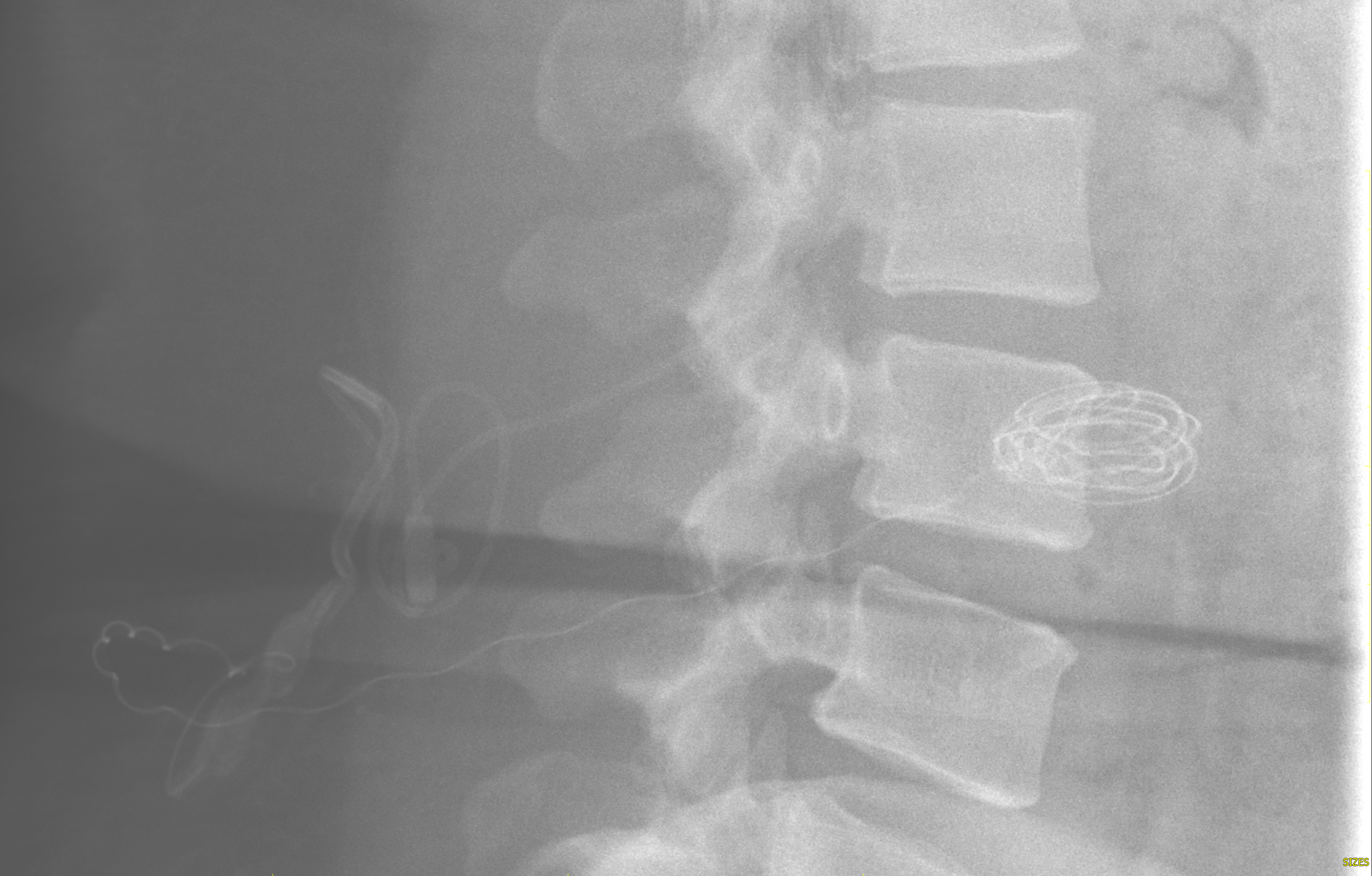
An intact lumboperitoneal shunt is in situ, with the distal shunt coiling within the left flank soft tissues.
The shunt's superior (proximal) intrathecal tip is poorly identified but projects at approximately T12 vertebral level.
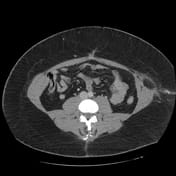



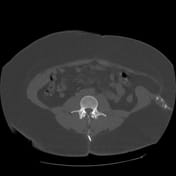

CT imaging confirms an intact lumboperitoneal shunt with an approximate T12 intrathecal access.
The distal shunt coils within the left flank soft tissues, with an associated non-calcified granuloma. The distal shunt tip is confirmed to be extraperitoneal, i.e., it does not penetrate the abdominal or pelvic cavity. No associated circumscribed hematoma, abscess, collection, or pseudocyst is present.
There is a left Spigelian hernia.
There are prominent extraskeletal adipose tissue consistent with an elevated BMI.
Case Discussion
This is an example of an unusual lumboperitoneal shunt malfunction. The intact shunt is coiled within the extraperitoneal left flank soft tissues and does not penetrate the abdominal or pelvic cavity. This is postulated as a shunt insertion error and likely occurred during insertion. The increased left flank adiposity in a setting of an elevated BMI contributed to the superficial placement, and the coiling likely occurred during the continued threading of the shunt at the time of insertion.
Shunt tip dislodgement and retraction are considered unlikely. There were no shunt tip complications other than an associated granuloma.
The patient was planned for shunt revision due to the imaging findings and ongoing symptoms.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.