
Presentation
Urinary urgency and frequency with high PSA level. No bony pain or weight loss.
Patient Data








Selected images from a skeletal survey: Ill-defined sclerotic lesions in the proximal left humerus and mid left femur; Ill-defined radiolucent lesion in the distal left femur; No obvious focal lesion in the dorso-lumbar spine and pelvic bones.
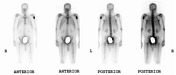
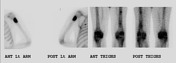
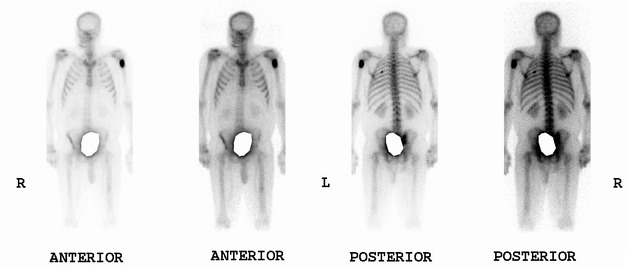
Abnormal focal radiotracer uptake in the proximal shaft of the left humerus, left 5th rib posteriorly and mid & distal shafts of the left femur. The rest of the skeleton shows homogeneous radiotracer distribution. Kidneys are visualized normally.





Increased bone density (osteoblastic metastases) of the visualized dorsolumbar spine, pelvic bones, proximal left femur and bilateral humeri (more on the left). No features of bowel obstruction or perforation are seen. A suprapubic catheter is seen in place. Asymmetry in the lumbar spine which is likely positional in nature.



Multiple areas of abnormal radiotracer uptake randomly distributed throughout the skeleton including right mastoid process, cervical and dorsolumbar spine, bilateral ribs, both sacroiliac joints, right iliac & ischium; left femoral head, neck & intertrochanteric area, and both humeral & femoral shafts. Poor visualization of both kidneys (superscan). Comparison with the previous scan shows disease progression.
Case Discussion
At initial presentation, review of slides and blocks of prostatic core biopsies (done in another hospital) showed prostatic adenocarcinoma in all core biopsies. Gleason grade = 7a (3 + 4). Perineural invasion: identified in core biopsy of right mid prostate. Lymphovascular space invasion: not identified.
Baseline PSA level was 11 ug/L (reference range ≤4 ug/L) which increased progressively during the follow up and after two years, the PSA level was 640 ug/L.
Follow up radiographs and bone scan showed progressive bone disease.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.