
Presentation
Increasing mid-chest pleuritic pain since endoscopic esophageal dilatation ?perforation.
Patient Data
Age: 16 years
Gender: Female
From the case:
Esophageal perforation
Download
Info
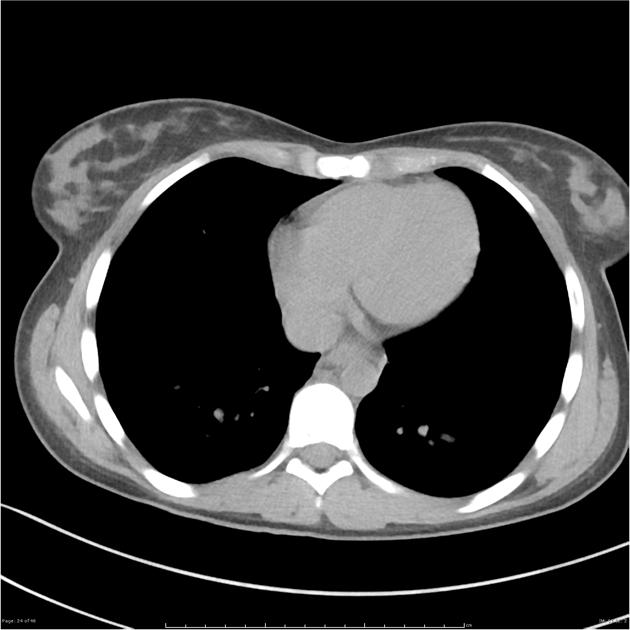
Small locule of gas is present outside the esophageal lumen, posterolateral to the caudate lobe of the liver. No other abnormal findings.
Download
Info
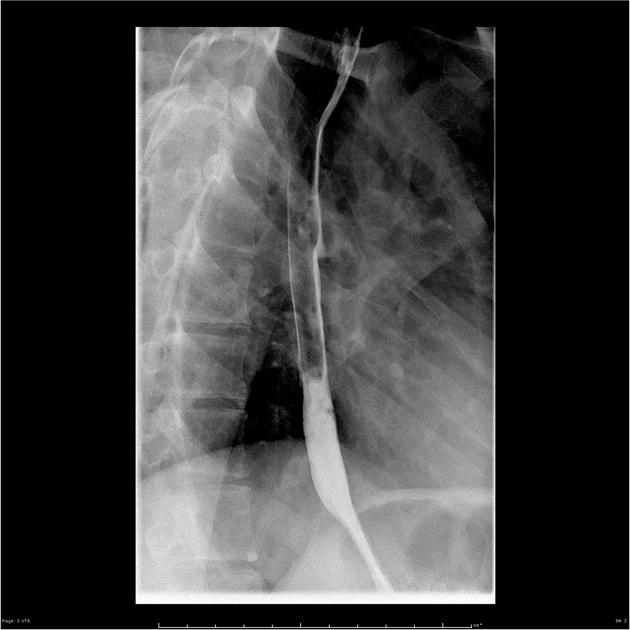
Mucosal irregularity of the anterior wall of the mid thoracic esophagus likely corresponds to the region of dilatation and represents a likely mucosal tear.
Acknowledgment: Dr David Wang.
Case Discussion
The evidence for esophageal perforation, a small locule of gas on CT and mucosal irregularity on fluoroscopic contrast swallow, is subtle but present in this case. Esophageal perforation is key to regonise because there is a mortality rate of ~20%.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.