
Presentation
The patient presented with rectal bleeding, anal pain, and passage of stool through the vagina. There is a history of rectal cancer, but no treatment has been undertaken.
Patient Data
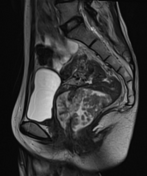











Irregular thickening of the wall of the lower rectum, demonstrating restricted diffusion and heterogeneous intense enhancement post-contrast, compatible with a primary malignant lesion (known rectal cancer). The lesion extends anteriorly with invasion into and communication with the vagina, resulting in a rectovaginal fistula.
There is involvement of the left levator ani muscle, mesorectal fascia, and extramural vascular invasion.
Approximately four suspicious lymph nodes are noted within and beyond the mesorectal fascia, with a maximum diameter of ~8 mm; the nodes appear round, show restricted diffusion, and enhance avidly post-contrast.
A few small-sized uterine fibroids are incidentally noted.
Case Discussion
Imaging findings are consistent with a rectovaginal fistula secondary to low rectal cancer invading the posterior vaginal wall. This is considered the most common type of gastrointestinal fistula involving the female genital tract.
Etiologies include obstetric complications, inflammatory bowel disease, postoperative causes, pelvic malignancies, trauma, infections, and various other factors.
Pelvic malignant tumors can lead to tissue destruction and fistula formation, as demonstrated in this case.
Features are suggestive of T4bN2aMx rectal carcinoma (with invasion of the vagina and left levator ani muscle), with positive circumferential resection margin (CRM ) and extramural vascular invasion (EMVI).


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.