
Presentation
2 weeks left lower chest pain radiating to the back. Severe hypertension. No past medical history.
Patient Data

Large well-circumscribed mass in the left hemithorax displacing the left lower lobe bronchus.
Otherwise normal lungs.
Normal left and right cardiac borders.
Normal chest wall.


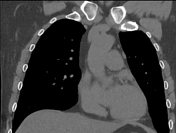


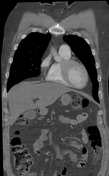


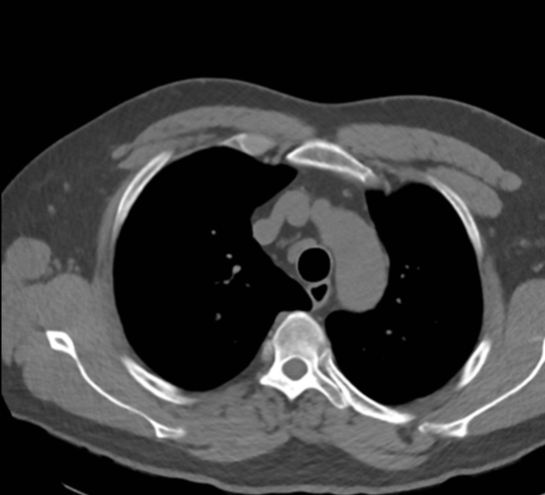
Large fusiform descending thoracic aortic aneurysm is seen, measuring 115 x 100 mm axially, and 125 mm in length. There is circumferential intraluminal thrombus up to 25mm in depth coating the partially calcified intima.
The aneurysm displaces/compresses the left main bronchus superiorly (coronal, sagittal), the left pulmonary artery (axial, coronal, sagittal) and the left pulmonary veins. There is adjacent compressive atelectasis of the posterior lingula and adjacent left lower lobe.
No posterior mediastinal or retroperitoneal fluid attenuation to suggest aneurysmal rupture. No evidence of intramural hematoma on the non-contrast phase. No intimal flap to suggest acute aortic dissection.
Normal appearance of the aortic root, aortic valve, bilateral coronary arteries, ascending aorta and aortic arch. The abdominal aorta and its branches are normal.
Conclusion
Large descending thoracic aortic aneurysm at high risk of rupture - urgent vascular and cardiothoracic review is suggested. No evidence of acute aortic syndrome.
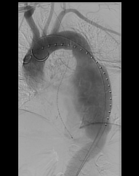
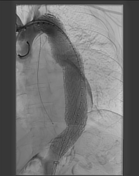

Thoracic endovascular aortic repair (TEVAR) was performed
Case Discussion
This patient had undiagnosed and unmedicated severe hypertension with a systolic blood pressure on admission of >190 mmHg. His ECG and bloods including cardiac troponin were normal. He was found to have a large descending thoracic aortic aneurysm (TAA), a major complication of chronic hypertension.
Although there were no imaging features of an acute event (acute aortic syndrome), the pain could indicate acute enlargement or mass effect. An aneurysm of this size is at risk of imminent rupture.
Urgent thoracic endovascular aortic repair (TEVAR) was performed by the vascular surgeons after a few days of observation in the intensive care unit. The patient suffered a large thromboembolic stroke post-operatively but made good neurological recovery with rehabilitation.
Aortic aneurysms can be categorized based on location into thoracic (TAA, inccidence 0.16%) and abdominal (AAA, incidence 4%) 1. The prevalence of TAA by location is 77% ascending, 5% arch, 10% descending and 8% thoracoabdominal 2.
A retrospective analysis of 1,326 patients with TAAs noted a mean aortic diameter of 52 mm at time of diagnosis. It was found that the risk of both TAA rupture and aortic dissection increase linearly with increasing aortic diameter 2. The risk of death after TAA rupture is as high as 97% 3.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.