
Presentation
Tetralogy of Fallot. Surgically-corrected VSD and bioprosthetic pulmonary valve. Presented with shortness of breath. Underwent a second pulmonary valve replacement.
Patient Data
Age: 20 years
Gender: Male

Download
Info
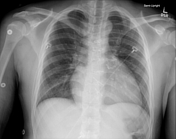
CXR 1
Original Carpentier-Edwards valve. Sternotomy wires of two kinds.
Ventricular septal defect (VSD) repair first.
Bioprosthetic valve in a right ventricular outflow tract (RVOT) conduit.
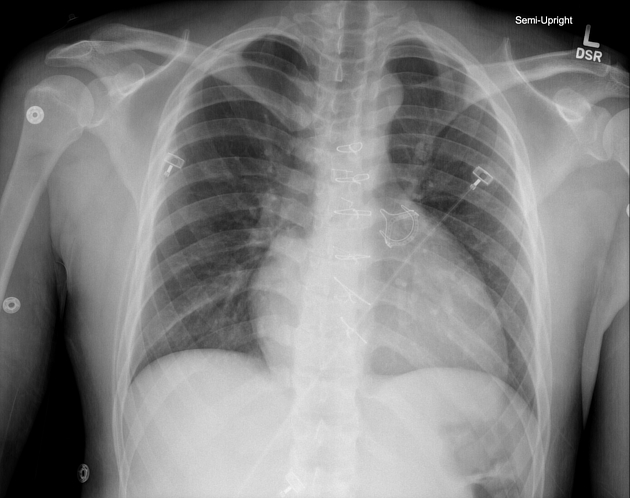
CXR 2
Postoperative image showing the percutaneously placed pulmonary valve on top of the older valve.
Case Discussion
Conclusions of cardiac MRI prior to transcatheter pulmonary valve replacement:
- patient born with tetralogy of Fallot. Surgically corrected VSD and prosthetic pulmonary valve are seen. 5-vessel aortic arch with a retroesophageal course of the right subclavian artery arising from the descending thoracic aorta.
- RVOT measures 38 mm in its maximal dimension. The main pulmonary artery measures 24 mm in maximal dimension. Right and left pulmonary arteries measure 21 and 24 mm in diameter.
- right ventricle: right ventricular dilatation, right ventricular hypertrophy, RV end diastolic volume index at least 135 mL. RV ejection fraction 53%.
- valvular function: severe pulmonary regurgitation of the prosthetic pulmonary valve (57%).
- delayed enhancement: none seen.
Therefore a transcatheter valve has been placed due to evidence of failure of the original valve.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.