
Gastroparesis (plural: gastropareses) is a functional gastric disorder caused by abnormal gastric motility with delayed stomach emptying in the absence of mechanical obstruction and results in gastric distension.
On this page:
Clinical presentation
Commonly presents with nausea, vomiting, postprandial fullness, early satiety, weight loss and/or weight gain and epigastric pain.
Pathology
Etiology
The most common etiologies are 1:
idiopathic
post-surgical: e.g. vagotomy, gastric fundoplication, gastric bypass surgery
medications: e.g. opiates, calcium channel blockers, alcohol
infection: e.g. Chagas disease, Clostridium botulinum
Radiological features
Plain radiograph
marked enlargement of gas-filled gastric bubble
Fluoroscopy
Upper GI barium study
A study of 50 patients with gastroparesis over an 8-year period found the following signs 2:
decreased or absent gastric peristalsis
gastric dilatation and delayed emptying of barium
debris/barium bezoar and retained fluid
Ultrasound
measuring emptying of a liquid meal by serially evaluating cross-sectional changes in the volume of the gastric antrum
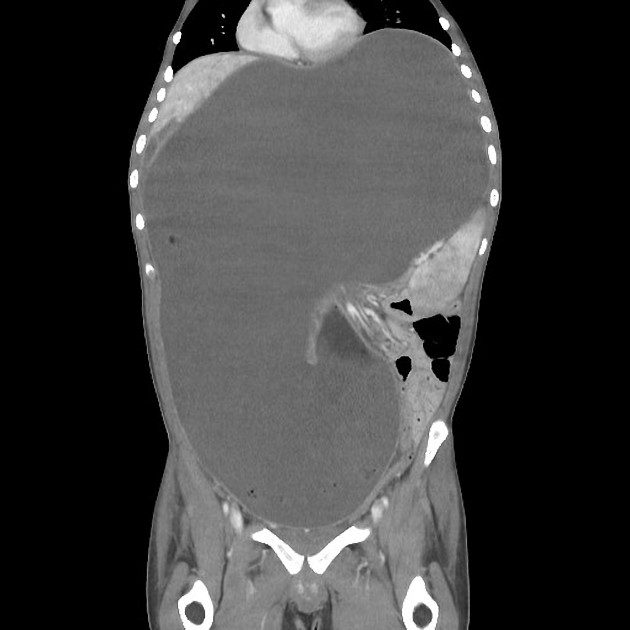
CT
marked gastric dilatation in the absence of mechanical obstruction or gastric masses
Nuclear medicine
The gold standard of diagnosis is solid meal gastric scintigraphy 3,4. Egg albumin radiolabelled with 37 MBq Tc-99m sulfur colloid is generally used and administered orally with toasted bread as an egg sandwich.
Measuring simultaneous solid and liquid emptying can be done with a liquid phase, in which water is labeled with 3.7 MBq In-111 DTPA. Data acquisition is performed for 60-120 minutes. Measurement of the half-emptying time is the simplest way to assess gastric transit.
Treatment and prognosis
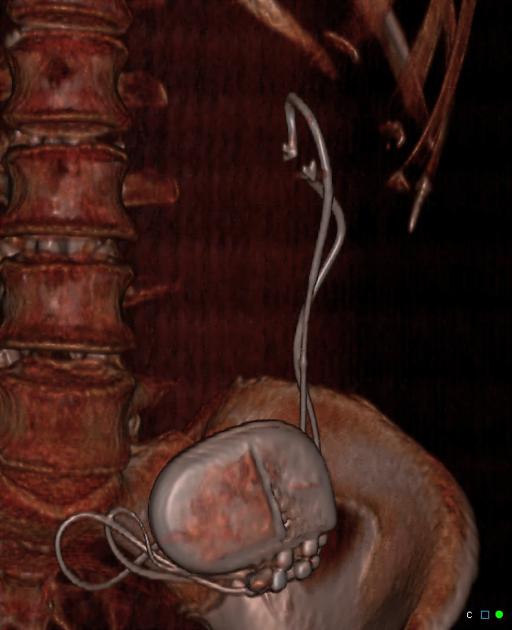
Management includes dietary modification, prokinetic and antiemetic medications, and surgical interventions. Gastric electrical stimulation techniques have been introduced (gastric pacemaker).
Differential diagnosis
gallstones (Bouveret syndrome)
duodenal or gastric peptic ulcers



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.