
Atypical lipomatous tumour / well-differentiated liposarcoma (ALT/WDLPS)
Updates to Article Attributes
Well-differentiated liposarcomas (WDLPS) or atypical lipomatous tumours (ALT) are locally aggressive adipocytic soft tissue neoplasms and are the most common form of liposarcomas.
Terminology
Atypical lipomatous tumours/well-differentiated liposarcomas (ALT/WDLPS) are also termed ‘atypical lipomas’, but this term has been discouraged 1.
Epidemiology
Atypical lipomatous tumours or well-differentiated liposarcomas account for 40-45% of liposarcomas and constitute the largest subgroup of adipocyte malignancies. They occur mostly in adults with a peak incidence in the 30s and 40s. In childhood, they are extremely rare. Inguinal lesions are more common in men otherwise there is no gender predominance however 1-3.
Associations
Atypical lipomatous tumours/well-differentiated liposarcomas may be associated with Li-Fraumeni syndrome 1.
Diagnosis
The diagnosis of well-differentiated liposarcoma is based on typical pathological features.
Diagnostic criteria
Diagnostic criteria according to the WHO classification of soft tissue tumours (blue book) differ with the subtype 1:
lipoma-like subtype:
- varying size of adipose cells
- nuclear atypia in adipose or stromal cells
sclerosing subtype:
- bizarre hyperchromatic stromal cells in a fibrillary collagenous stroma
inflammatory subtype:
- atypical stromal cells in a chronic inflammatory infiltrate
The following criteria are described as desirable in challenging cases 1:
- MDM2 and/or CDK4 nuclear expression
- MDM2 and/or CDK4 gene amplification
Clinical presentation
The most common presentation is that of a painless mass. Deep-seated atypical lipomatous tumours/well-differentiated liposarcomas are most often found incidentally 1.
Complications
If left untreated atypical lipomatous tumours/well-differentiated liposarcomas can dedifferentiate into higher-grade malignancies such as dedifferentiated liposarcoma or undifferentiated pleomorphic sarcoma 1-4.
Pathology
Atypical lipomatous tumours/well-differentiated liposarcomas are adipocytic neoplasms characterized by a proliferation of pleomorphic mature adipocytes of different patterns featuring atypical hyperchromatic stromal cells. They are intersected by fibrous septa, might have myxoid or fibrous components and areas of fat necrosis 1-4.
Location
Atypical lipomatous tumours/well-differentiated liposarcomas commonly involve the deep soft tissues in particular of the proximal extremities and the trunk 1-5.
Common locations include the following 1:
- thigh and buttocks
- shoulder and back
- retroperitoneum
- paratesticular area
Rarer locations of involvement include the following 1:
- head and neck
- mediastinum
- distal extremities
- skin
Classification
Atypical lipomatous tumours/well-differentiated liposarcomas include the following subtypes 1-4,6:
- lipoma-like liposarcoma
- sclerosing liposarcoma
- inflammatory liposarcoma
Macroscopic appearance
Macroscopically atypical lipomatous tumours/well-differentiated liposarcomas usually present as well-circumscribed, large lobulated masses of variable consistency and white to yellowish colour. They might display foci of necrosis or small punctate haemorrhages 1.
Microscopic appearance
The microscopic appearance of atypical lipomatous tumours/well-differentiated liposarcomas includes the following features. Larger tumours and especially retroperitoneal tumours commonly show more than one morphologic pattern within the same lesion1,4:
- presence of atypical hyperchromatic stromal cells
- variable number of lipoblasts
- possibly variations in adipocyte size with nuclear atypia (lipoma-like subtype)
- possibly copious inflammatory infiltrates (inflammatory subtype)
- possibly bizarre stromal cells within a fibrillary sclerotic, collagenous background (sclerosing subtype)
Immunohistochemistry
Immunohistochemistry stains are usually positive MDM2 and/or CDK4 1.
Genetics
The pathogenesis of atypical lipomatous tumours/well-differentiated liposarcomas involves MDM2 and/or CDK4 nuclear gene amplification 1,2.
Diagnosis
The diagnosis of well-differentiated liposarcoma is based on typical pathological features.
Diagnostic criteria
Diagnostic criteria according to the WHO classification of bone tumours (blue book) differ with the subtype 1:
lipoma-like subtype:
varying size of adipose cellsnuclear atypia in adipose or stromal cells
sclerosing subtype:
bizarre hyperchromatic stromal cells in a fibrillary collagenous stroma
inflammatory subtype:
atypical stromal cells in a chronic inflammatory infiltrate
The following criteria are described as desirable in challenging cases 1:
MDM2 and/or CDK4 nuclear expression-
MDM2and/orCDK4gene amplification
Radiographic features
Imaging features of atypical lipomatous tumours/well-differentiated liposarcomas resemble that of benign lipomas as discussed in the article lipoma vs well-differentiated liposarcoma and include 3-5:
- size > 5 cm
- thick or nodular septae (>2 mm) with possible enhancement
- multinodular tumour margins
- focal nodular patchy non-fatty tissue components
- more than ¾ of fatty tissue
They might displace other organs or tissue.
Ultrasound
Usually appears as multilobulated well-defined mass sometimes with hyperechoic foci 3.
CT
CT usually shows a fat tissue density mass with thick or nodular enhancing septae. Calcifications might be rarely found 4.
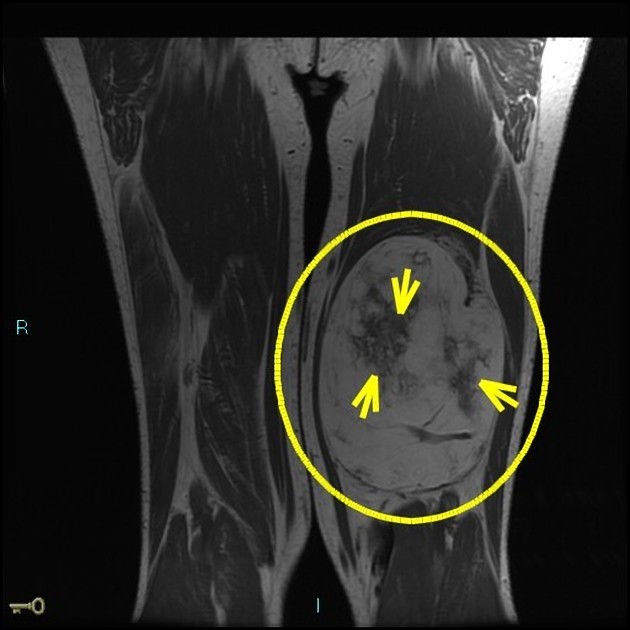
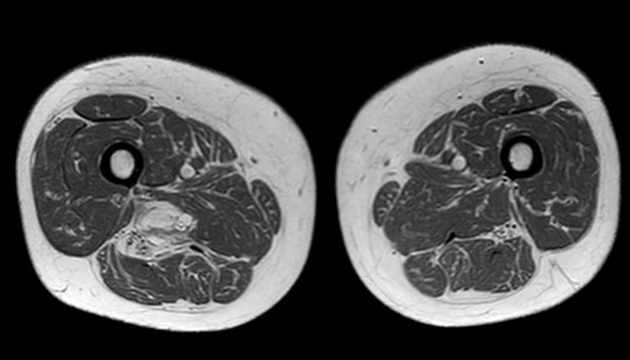
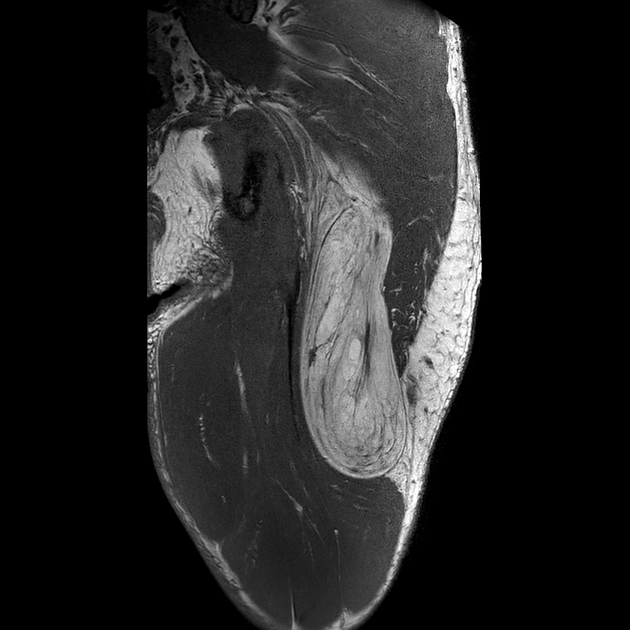
MRI
On MRI atypical lipomatous tumours/well-differentiated liposarcomas will display a mass of fat isointense signal in all sequences. In addition, atypical lipomatous tumours/well-differentiated liposarcomas will show thick septae or nodular non-lipomatous areas with contrast enhancement 3-5.
- T1: hyperintense
- T2: hyperintense possibly with prominent high signal foci
- T2FS/PDFS: hypointense
- T1 C+ (Gd): moderate to markedenhancement of septae
Radiology report
The radiological report should include a description of the following 5:
- form, location and size
- tumour margins
- thick septae and septal enhancement
- amount of non-adipose tissue
- distance from the muscular fascia
- relationship to local nerves and vessels
Treatment and prognosis
The management of choice in atypical lipomatous tumours/well-differentiated liposarcomas is resection, which is curative if complete 1. The tumours are not sensitive to radiotherapy or chemotherapy 2. Tumour prognosis is therefore mostly dependent on how amenable the location is to surgical excision. The tumour does not cause distant metastasis unless there is dedifferentiation. Therefore tumours of the mediastinum retroperitoneum or spermatic cord have a worse prognosis, due to their location they are more prone to local recurrence 1,2.
Differential diagnosis
Conditions or tumours which can mimic the presentation and/or the appearance of atypical lipomatous tumours/well-differentiated liposarcomas include 1-5:
- lipoma e.g. intermuscular/intramuscular lipoma
- lipomatosis
- myxoid liposarcoma
- dedifferentiated liposarcoma
- myolipoma
- angiomyolipoma
- fibrolipomatosis
- spindle cell/pleomorphic lipoma
- hibernoma
- fat necrosis




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.