
Osteonecrosis of the femoral head, previously known as avascular necrosis (AVN) of the hip, is the most common site for osteonecrosis, presumably due to a combination of precarious blood supply and high loading when standing.
Idiopathic osteonecrosis of the femoral head epiphysis in children (Perthes disease) is typically considered separately; thus the remainder of the article pertains to osteonecrosis in the skeletally mature population.
On this page:
Epidemiology
Typically affects adults under 50 years of age 12.
Clinical presentation
The most common presenting symptom is pain in the region of the affected hip, thigh, groin, and buttock. However, few patients may remain asymptomatic until the late stages.
Pathology
Typically it affects the superior articular surface (between 10-2 o'clock) and begins in the most anterior part of the hip.
Etiology
It can be thought of as traumatic (secondary to the neck of femur fractures) or non-traumatic. Traumatic osteonecrosis is usually unilateral 10. In non-traumatic cases, it is mostly bilateral in 70-80% 10.
traumatic
chronic corticosteroid therapy
alcohol use
smoking
Radiographic features
Other than describing the general appearance of the affected region, the following are necessary to include in the report as they have a bearing on prognosis and treatment:
position
estimating percentage volume of the head involved (axial) and percentage weight-bearing surface involved (coronal)
coexisting osteoarthritis or secondary degenerative change
joint effusion
presence of a potentially unstable osteochondral fragment: rim sign
CT
CT is often more sensitive than plain film in showing subchondral fractures.
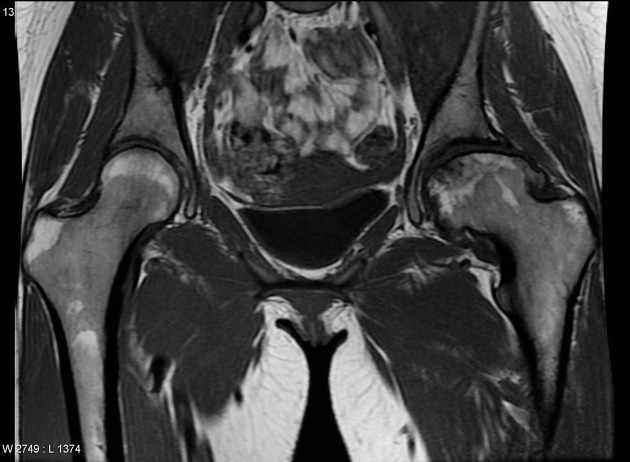
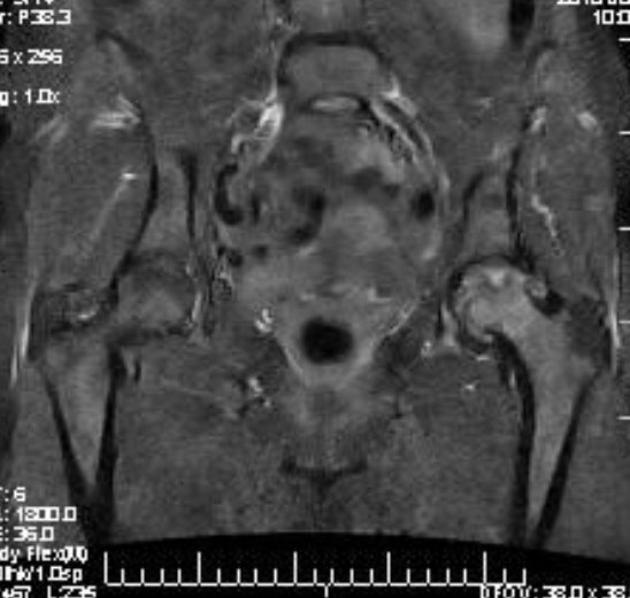
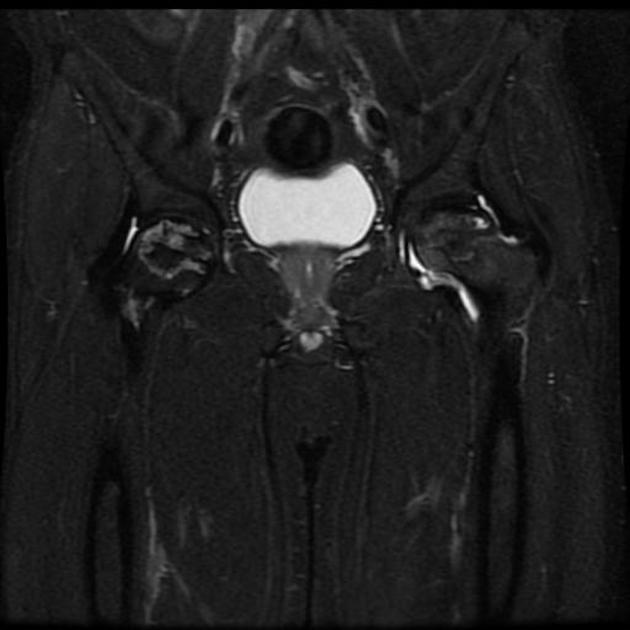
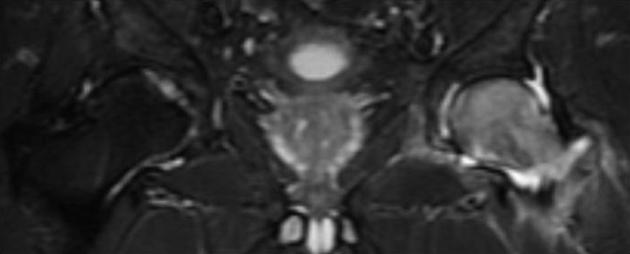
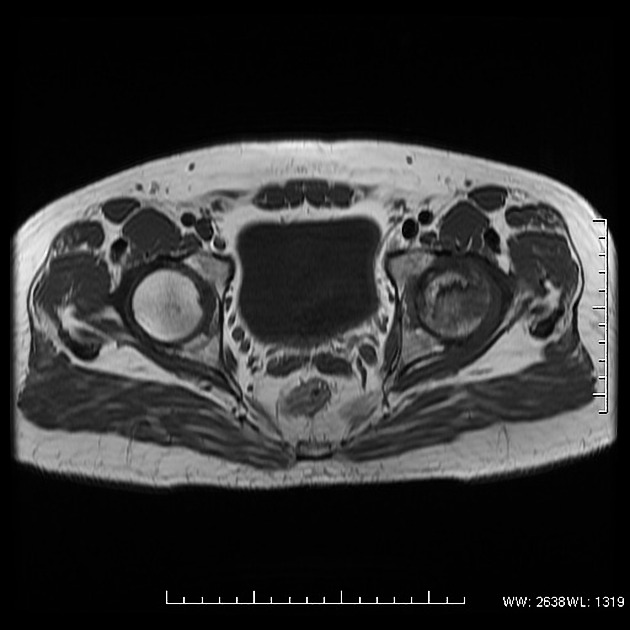
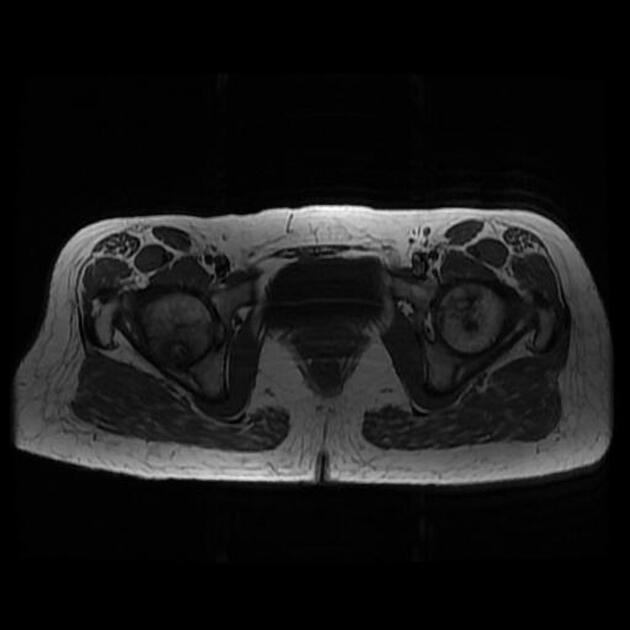
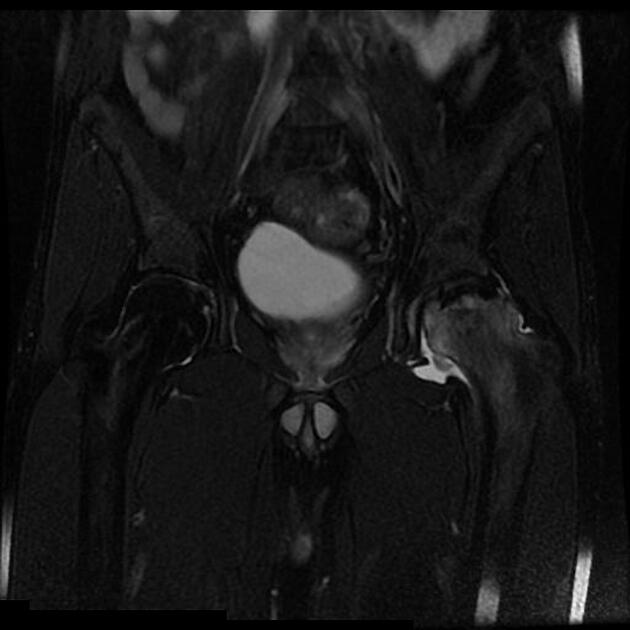
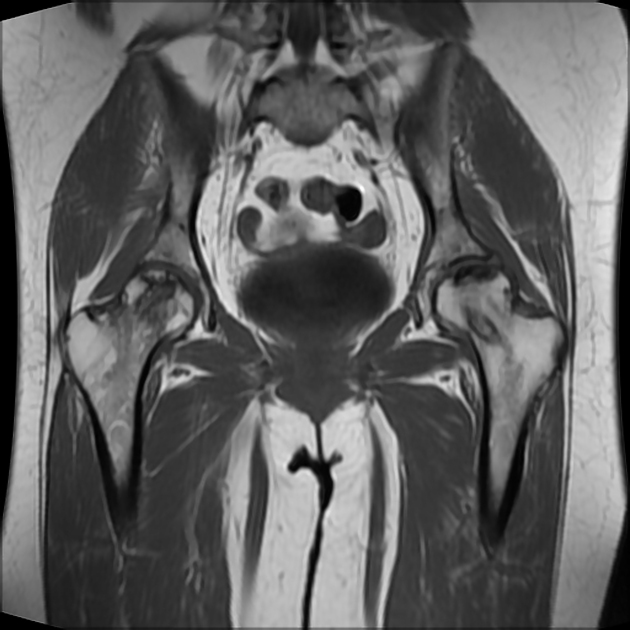
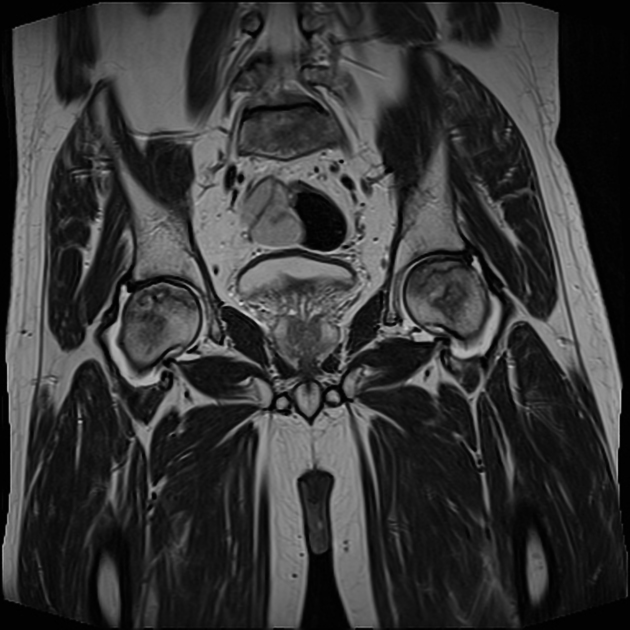
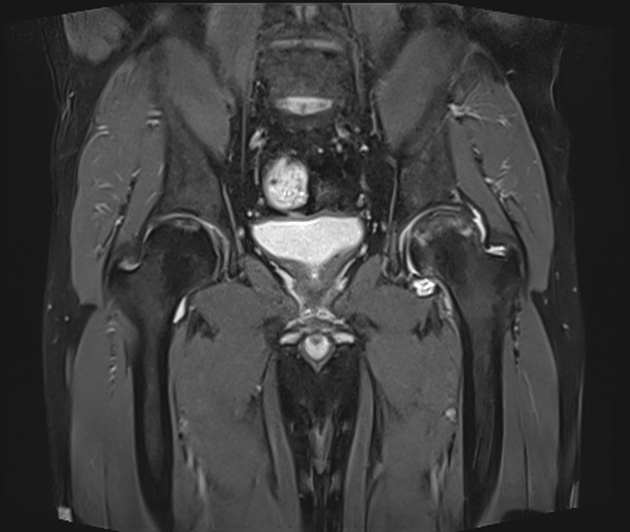
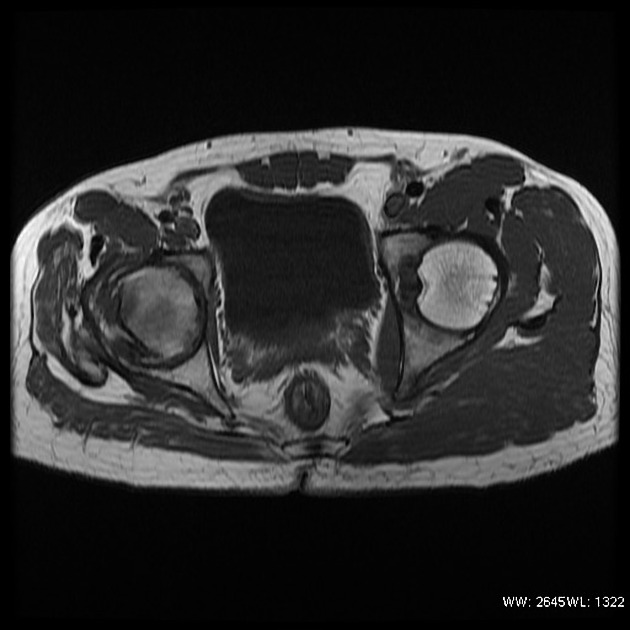
MRI
MRI is the most sensitive modality, with a sensitivity of 71-100% and specificity of 94-100% 1. As there is a high rate of bilateral involvement, both hips should be included in the field of view of at least some sequences.
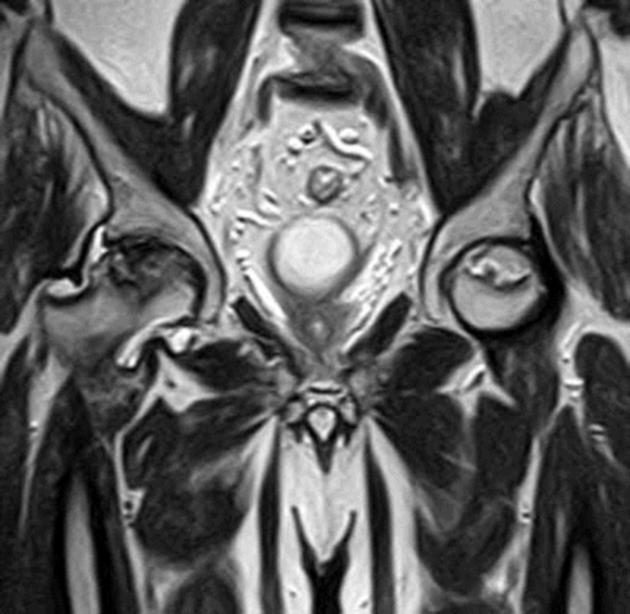
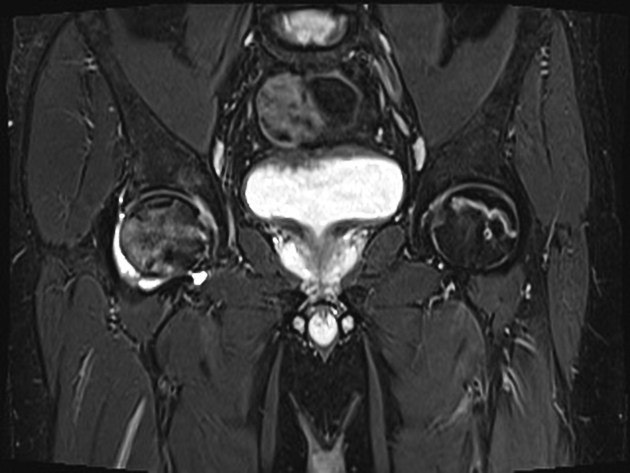
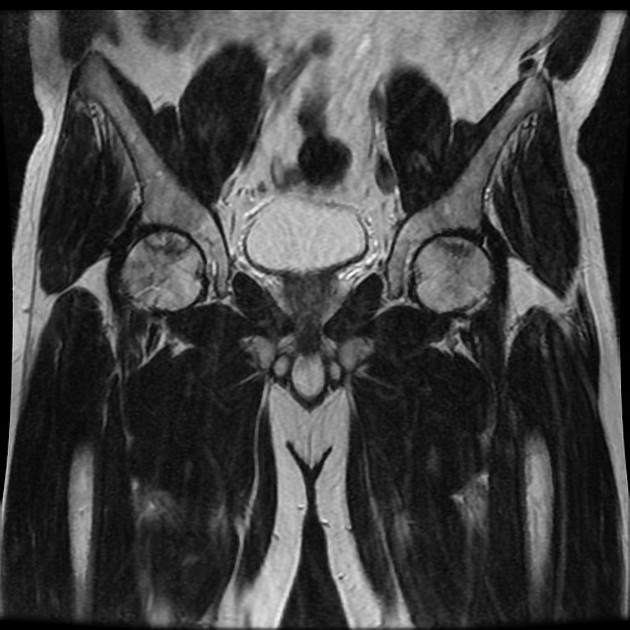
T1: usually the initial specific findings are areas of low signal intensity representing edema, which can be bordered by a hyperintense line that represents blood products
T2: may show a second hyperintense inner line between normal marrow and ischemic marrow; this appearance is highly specific for osteonecrosis of the hip and is known as the "double-line sign"
Staging
Several staging systems for osteonecrosis of the hip exist. The earliest and most commonly used is the Ficat and Arlet classification (1980) which includes x-ray, MRI and bone scan appearances. The Steinberg classification (1995) is similar but quantifies the involvement of the femoral head. The Mitchell classification (1987) is commonly utilized for MRI images. The ARCO classification (2019) encompasses both x-ray and MRI 10.
Differential diagnosis
In some situations consider:
subchondral insufficiency fracture of the femoral head: typically considered a different entity 9
General imaging differential considerations include:
hematopoietic marrow (see bone marrow)
-
idiopathic transient osteoporosis of the hip (ITOH)
hyperemia with diffuse increased uptake of radiotracer by the femoral head, neck, and intertrochanteric region
fracture
-
pain and fever
usually involves both sides of the joint





























 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.