
Central chondrosarcomas grade 2 and 3 (CS2/CS3) are malignant intermediate- and high-grade conventional chondrosarcomas that arise intramedullary 1-3.
On this page:
Epidemiology
Similar to low-grade chondrosarcoma, the incidence of central intermediate and high-grade chondrosarcomas has also risen compared to the 1990s and has been last estimated at 1.5-2 per million person-years 1,2.
Intermediate-grade to high-grade chondrosarcomas are mainly found in the adult population in the third to the sixth decade with equal gender distribution 1, though patients with enchondromatosis are usually younger than patients with primary tumors 1.
Associations
Central chondrosarcomas are associated with enchondromatosis 1,4.
Diagnosis
A provisional diagnosis can be often made by a combination of clinical examination and imaging and is confirmed by histology.
Diagnostic criteria
Diagnostic criteria according to the WHO classification of soft tissue and bone tumors (5th edition) 1:
location in the bony medulla
cartilaginous tumor with a lobular growth pattern
entrapment of pre-existing lamellar trabecular bone
myxoid matrix
increased cellularity, presence of mitoses
no osteoid production of the malignant cells
Clinical presentation
Pain and/or swelling are common symptoms. Tumors growing from the pelvic bones or thoracic cage can grow quite large before they are discovered 1. They can also present with a pathological fracture 1. Chondrosarcomas of the skull base and spine can cause neurological symptoms 1.
Pathology
Intermediate- and high-grade chondrosarcomas grades 2 and 3 are malignant cartilage matrix-forming tumors arising from endochondral ossification 1. They can develop without or from a pre-existing precursor lesion.
Etiology
Individuals with enchondromatosis and a somatic mosaic mutation in IDH1 or IDH2 are at higher risk to develop chondrosarcomas 1.
Location
The most common sites are the following 1:
long tubular bones: especially proximal femur > proximal humerus > distal femur
flat bones: ileum most common
The spine and skull are occasionally affected 1.
Macroscopic appearance
Grossly, intermediate- to high-grade chondrosarcomas are characterized by the following features 1:
translucent grayish-blue or grey-white tissue cut surface
chalky yellow-white areas of calcification
cystic and myxoid changes
frequent cortical erosion, cortical destruction and soft tissue extension
Microscopic appearance
Microscopically, intermediate- to high-grade chondrosarcomas display the following histological features 1,6,7:
lobular growth pattern
entrapment of pre-existing lamellar bone (tumor around three sides of normal trabeculae)
chondroid matrix consisting of hyaline cartilage and a variable extent of myxoid changes
higher cellularity than low-grade chondrosarcoma
small condensed nuclei, variable nuclei with visible nucleoli
presence of mitoses especially in high-grade chondrosarcoma (grade 3), some nuclear atypia
frequent cortical destruction and breakthrough
mostly spindled and less differentiated cells in the periphery of high-grade tumors
Immunophenotype
Immunohistochemical staining is reactive for S100 and negative for brachyury. Only a small percentage of IDH mutations are recognized with limited use 1.
Genetics
About 50% of chondrosarcomas display somatic mutations in the IDH1 and IDH2 genes 1. They are also characterized by aneuploidy and complex karyotypes as well as alterations in the p53 and RB1 signaling pathways in >80% of high-grade chondrosarcomas 7. Other alterations include mutations in the COL2A1 gene in more than one-third of the cases 7,8. Copy number variations of CDKN2A are found in about ¾ of high-grade central chondrosarcomas, but not in low-grade chondrosarcomas or enchondromas 1,7.
Radiographic features
General radiographic features of central intermediate and high-grade chondrosarcomas include 9-12:
lesion size >5 cm
lobulated osteolytic growth
cortical destruction
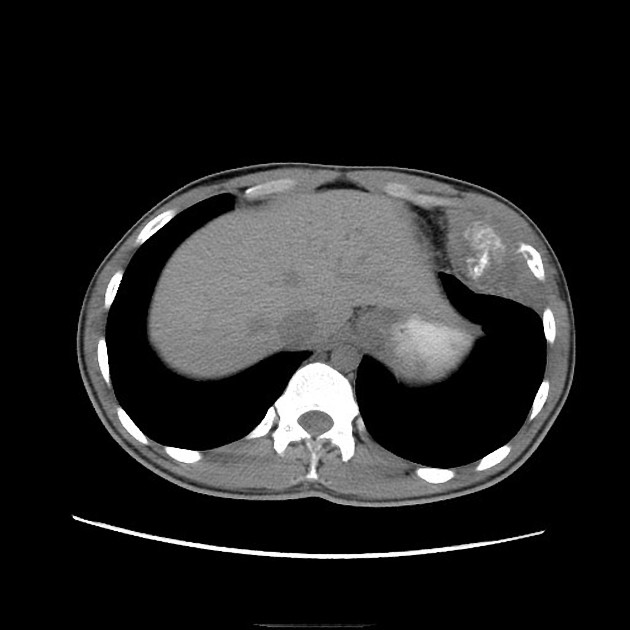
Plain radiograph/CT
Radiographic features of low-grade chondrosarcomas include the following 1:
lytic lesion
geographical, lobulated shape
expansile remodeling, cortical thickening and periosteal reaction
ill-defined margins with moth-eaten or permeative bone destruction
intralesional calcifications: (rings and arcs calcification or popcorn calcification)
On CT imaging features are the same as on plain radiographs but are more readily seen and better assessable.
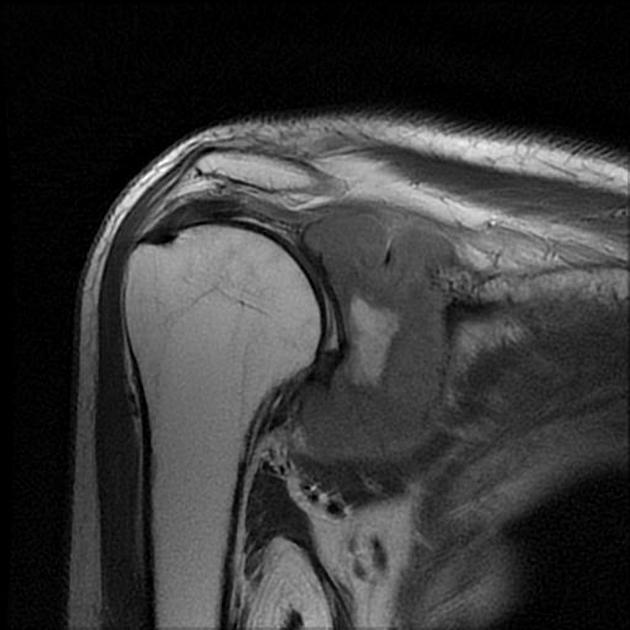
MRI
MRI is an important tool in the detection, grading and differentiation of intermediate- to higher-grade chondrosarcomas versus low-grade chondrosarcoma as well as other bone tumors. MR imaging characteristics include the following 1,9-16:
intramedullary location, lobulated or geographical shape
abundant mucoid changes (>50%) with fluid signal intensity on all sequences 11
absence or loss of entrapped fatty marrow 10 (e.g. on follow-up studies)
bone expansion, cortical thickening and cortical destruction
peritumoral bone marrow edema and soft tissue edema
periostitis 13
soft tissue extension
intralesional hemorrhage or necrosis 15
It is important to realize typical imaging features of cartilaginous tumors such as lobulated growth patterns and the rings and arcs appearance can become lost due to poor cell differentiation in higher-grade tumors 12.
The clinical utility of diffusion-weighted imaging in the evaluation of intermediate to high-grade chondrosarcoma remains inconclusive 10.
Also of note is, that there are no particular MR imaging features predictive in small bones 14.
Signal characteristics
T1: low to an intermediate signal
T2: high intensity with or without signal voids indicating calcifications
GRE/SWI: blooming of mineralized/calcified portions
T1 C+ (Gd): peripheral and septal contrast enhancement 9
DCE: arterial enhancement favors chondrosarcoma vs enchondroma
Nuclear medicine
PET-CT can show a high FDG uptake in intermediate- and high-grade chondrosarcomas with a SUVmax of >4.4 and a high specificity of 99% versus enchondromas and low-grade chondrosarcomas 11,17, with the limitation that almost half of the intermediate and high-grade chondrosarcoma cases will reveal a SUVmax in an inconclusive range of 2-4.4 not helping the differentiation versus low-grade chondrosarcomas 1.
Radiology report
The radiological report should include a description of the following 10-16:
shape and size (especially >5 cm)
location (long bones, axial skeleton)
tumor margins and transition zone
absence or loss of entrapped fatty marrow and/or fat replacement (during follow-up) 12
expansile remodeling
cortical destruction/breach
periosteal reaction
soft tissue component
neurovascular involvement
Treatment and prognosis
Treatment consists of en bloc resection to achieve tumor-free margins 1,4. They are relatively resistant to radiotherapy 3. Local recurrences are more frequent than in low-grade chondrosarcomas and occur in about 19-26% 1 being more frequent in higher-grade tumors 1,2.
Overall survival rates for chondrosarcoma grade 2 (CS2) are in the range of 70-90% and 60-85% after 5 and 10 years and for chondrosarcoma grade 3 (CS3) 5-year and 10-year survival rates are in the range of 31-75% and 26-55% respectively 1,2,10,18,19.
The chance of metastasis is approximately 10-30% in intermediate-grade chondrosarcomas (CS2) and about 30-70% in high-grade chondrosarcomas 1.
Complications
The main complications include 1,
tumor recurrence
distant metastases
pre-operative histology carries the risk of tumor seeding within the biopsy tract 11
History and etymology
Chondrosarcomas were first described by the American bone pathologists Louis Liechtenstein and Henry Lewis Jaffe in 1939 20.
Intermediate and high-grade chondrosarcoma have been separated from low-grade chondrosarcoma since the fourth edition of the WHO classification of bone tumors in 2013 2,3,16,21.
Differential diagnosis
Conditions or tumors which can mimic the presentation and/or the appearance of central intermediate- to high-grade chondrosarcoma include 1,16:
central atypical cartilaginous tumor/chondrosarcoma grade 1 (ACT/CS1)
dedifferentiated chondrosarcoma (biphasic pattern on T2w imaging)






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.