
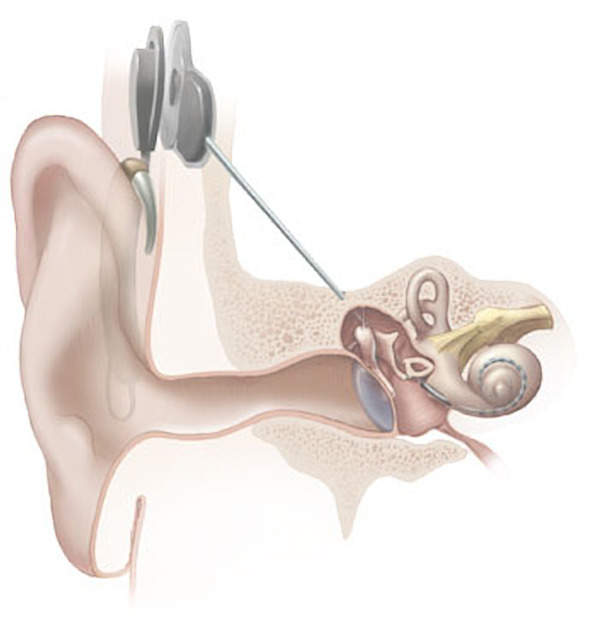
Cochlear implants (CI) are surgically implanted electronic device that provides a sense of sound to a person who is profoundly deaf or severely hard of hearing. Unlike conventional hearing aids, the cochlear implant does not amplify sound but works by directly stimulating any functioning auditory nerves inside the cochlea with an electric field.
External components of the cochlear implant include a microphone, a speech processor and a radiofrequency (RF) transducer or primary headpiece coil. A secondary coil is implanted beneath the scalp and inductively coupled to the primary headpiece coil.
The implant gives recipients additional auditory information, which may include sound discrimination fine enough to understand speech in quiet environments. Post-implantation rehabilitative therapy is often critical to ensuring successful outcomes.
Radiographic features
The electrodes should be intracochlear; the radial position of the tip determines the depth. Complications observed postoperatively include electrode 13:
-
tip fold over
can result in the rupture of the basilar membrane
-
basal fold over
fold over at the basal portion of the array
can result in the rupture of the basilar membrane
-
under-insertion or extrusion
electrode contacts are sitting outside of the cochlear
-
over-insertion
most proximal electrode contact is >3mm from the round window
kinking or pinching
-
scalar translocation
electrode is translocated from the scala tympani into the scala vestibuli
can result in basilar membrane injury
-
tympanic cavity placement
typically seen in the context of CHARGE syndrome where the array can't make the basal turn and sits in the tympanic cavity
placement in the internal auditory canal
placement in the vestibulum and semi-circular canals
Regular electrode
Before assessing post operative imaging it is important to note the route in which the implant has been inserted, it can be one of three ways via the 12:
round window (the preferred method)
extended round window (where the round window is enlarged and opened via drilling of the anterior-inferior margin)
cochleostomy
Split electrode
The split electrode (used in patients with otosclerosis) implant comprises two electrodes in the cochlear, one in the basal turn and one in the second turn.
Retrograde electrode
Patients with basal turn ossification require insertion via cochleostomy.
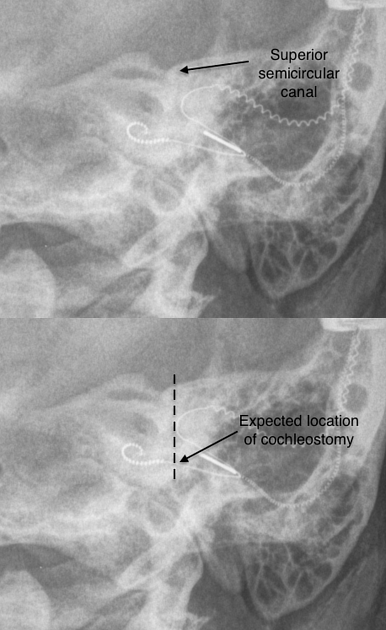
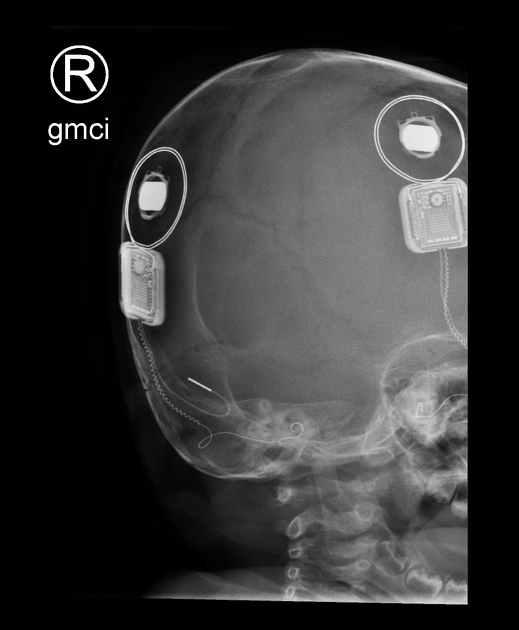
Plain radiograph
Post operative plain film radiography of the temporal bones are sufficient in a majority of patients. Plain radiography is the most helpful modality to assess for extrusion and superior in assessing the number of inserted electrodes. Typically a modified Stenvers view is performed, which has succeeded the original Stenvers view.
Correct placement of the electrodes are within the scala tympani regions 11
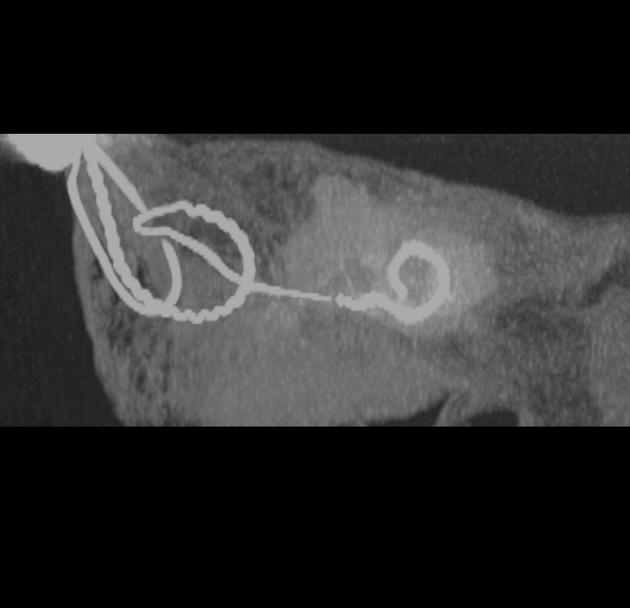
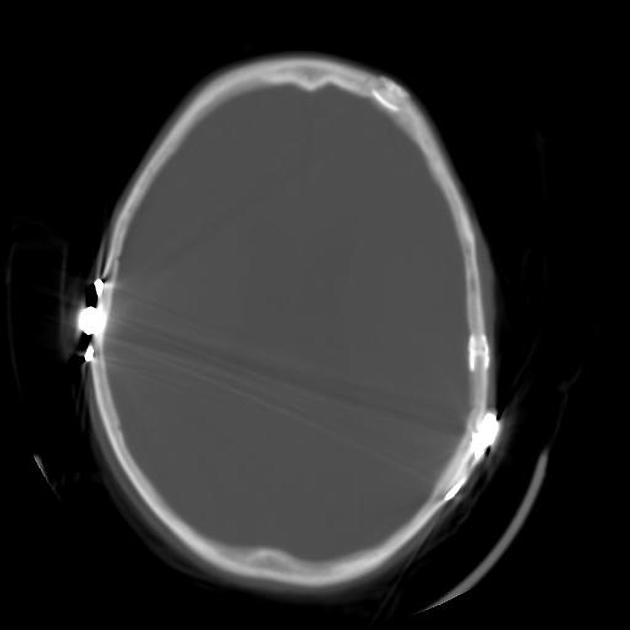
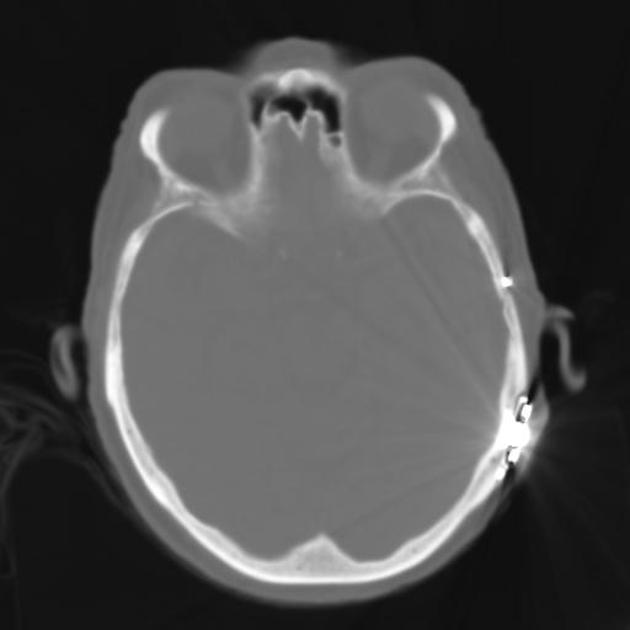
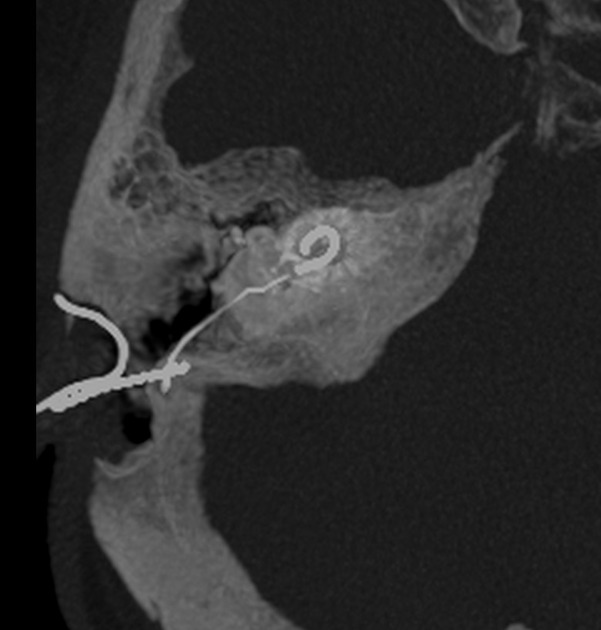
CT
Particularly useful when postoperative radiographs fail to demonstrate the location of the electrode array adequately or if postoperative infection is suspected 1.
Usually thin-collimation (≤1 mm) scanning performed contiguously or with a 0.5–1-mm overlap is required.







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.