
Duret hemorrhages are small, usually multiple, hemorrhages in the midbrain or pons resulting from rapidly developing brain herniation, especially central herniation. They generally have a dismal prognosis.
On this page:
Clinical presentation
The clinical presentation from Duret hemorrhages is difficult to discern due to the confounding effect from the significant other intracranial pathology that is causing the Duret hemorrhages (e.g. a large extra-axial hemorrhage). Most patients with Duret hemorrhages present with decreased conscious state, and in patients who survive to recovery, have residual focal neurological deficits 9,10.
Pathology
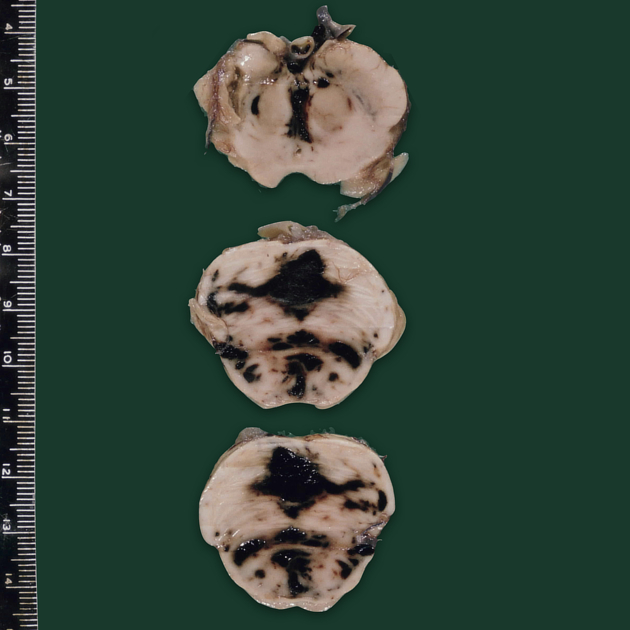
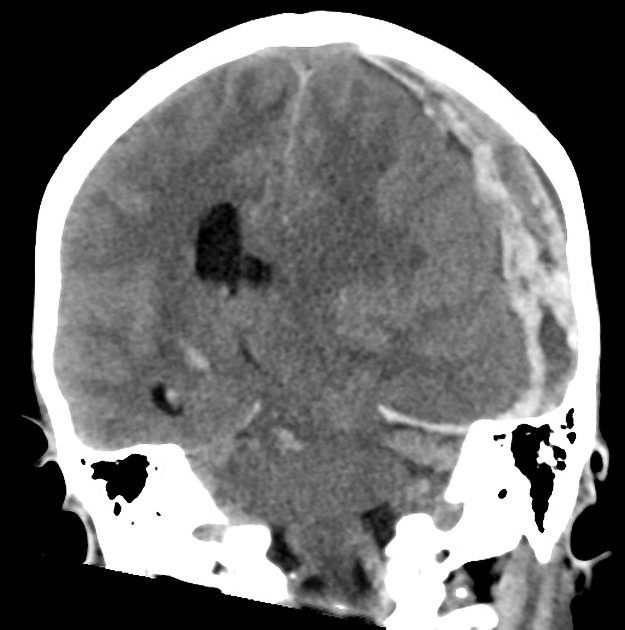
Raised supratentorial pressure causes the brainstem and mesial temporal lobes to be forced downwards through the tentorial hiatus. As a result of this shift, it is believed that perforating branches from the basilar artery and/or draining veins are damaged with resultant parenchymal hemorrhage. Most commonly it is seen in patients with severe herniation 12 to 24 hours prior to death 2.
Etiology
Duret hemorrhages are associated with descending transtentorial herniation, which can occur due to various underlying causes. Herniation syndromes manifest as a result of increased intracranial pressure, leading to shifts in intracranial compartments. The etiology of Duret hemorrhages include 8:
hyponatremia
following the administration of thrombolytics (rarely)
Radiographic features
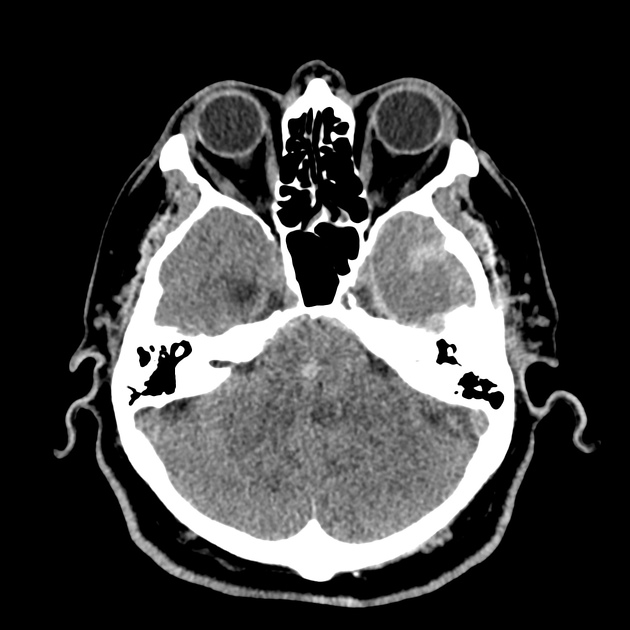
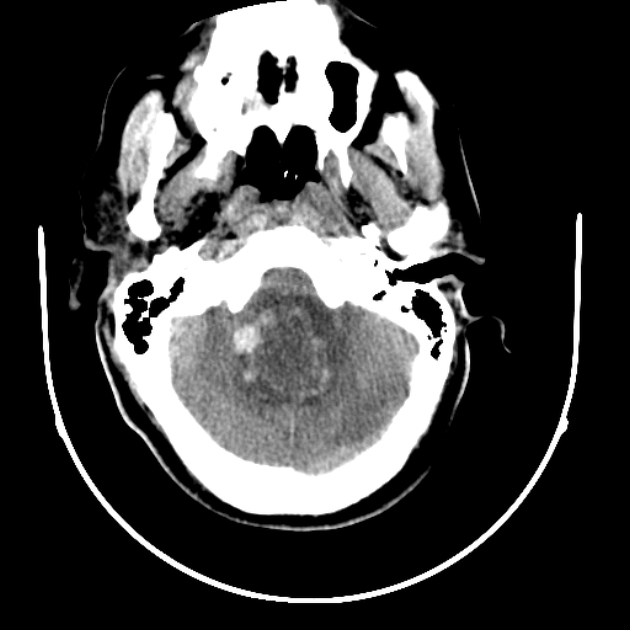
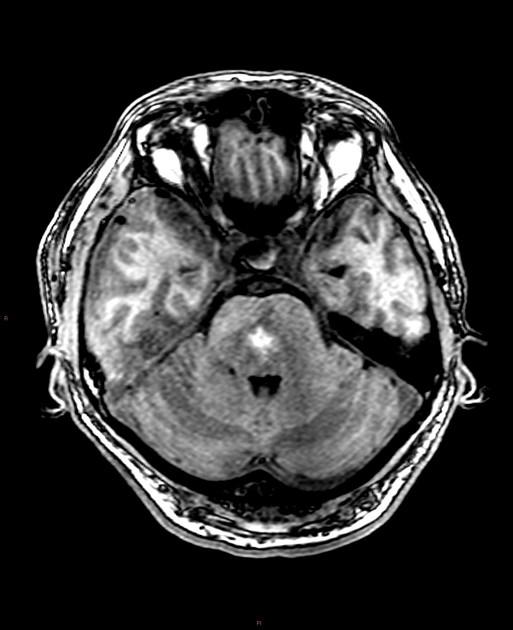
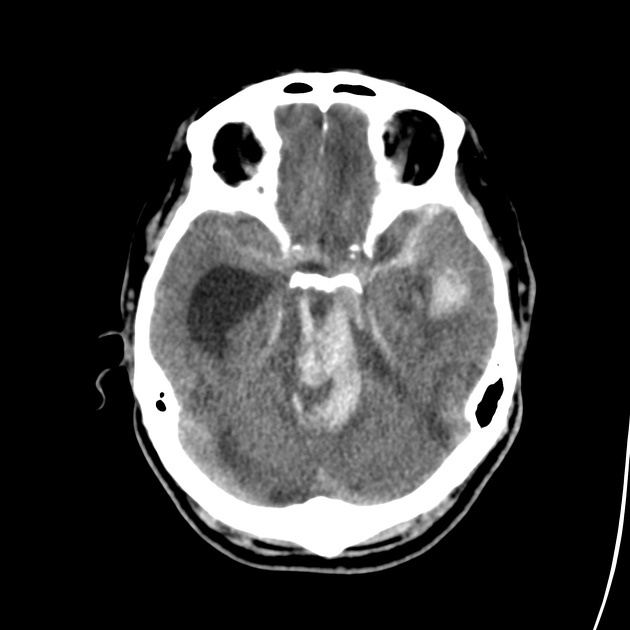
The classical appearance of a Duret hemorrhage is a single small, round hemorrhage located in the midline of the midbrain or pons near the pontomesencephalic junction 5. Often, however, these hemorrhages can be multiple or even extend into the cerebellar peduncles.
See the main article on intracerebral hemorrhage regarding further details of radiographic features.
Treatment and prognosis
Usually considered fatal in the majority of cases although occasional cases have been reported to have favorable outcomes 6,9,10.
History and etymology
It was first described by Henri Duret (1849-1921), a French surgeon, in 1874 4,7.
Differential diagnosis
On imaging consider:
-
primary hypertensive brainstem hemorrhage
usually larger
mid pons
absence of herniation initially (although hydrocephalus may well develop)
-
brainstem contusion/diffuse axonal injury
dorsal midbrain (tectum and periaqueductal grey matter)
usually multifocal and smaller







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}