
Foot radiographs are commonly performed in Emergency departments, usually after sport-related trauma and often with a clinical request that states lateral border pain. Remember to check the whole film, though. Often, a foot x-ray is also requested for the investigation of osteomyelitis, arthritides, or bone lesion.
This article relates mainly to traumatic injuries to the foot.
A basic review should start with AP and lateral views (including the entire foot and ankle). With the exception of trauma, these views should be acquired with weight bearing if the patient can tolerate it.
On this page:
Systematic review
Choosing a search strategy and utilizing it consistently is a helpful method to overcome common errors seen in diagnostic radiology. The order in which you interpret the radiograph is a personal preference. A recommended systematic checklist for reviewing musculoskeletal exams is soft tissue areas, cortical margins, trabecular patterns, bony alignment, joint congruency, and review areas. Review the entire radiograph, regardless of perceived difficulty. Upon identifying an abnormality, do not cease the review, put it to the side and ensure to complete the checklist.
Soft tissue
Assess all soft tissue structures for any associated or incidental soft tissue signs
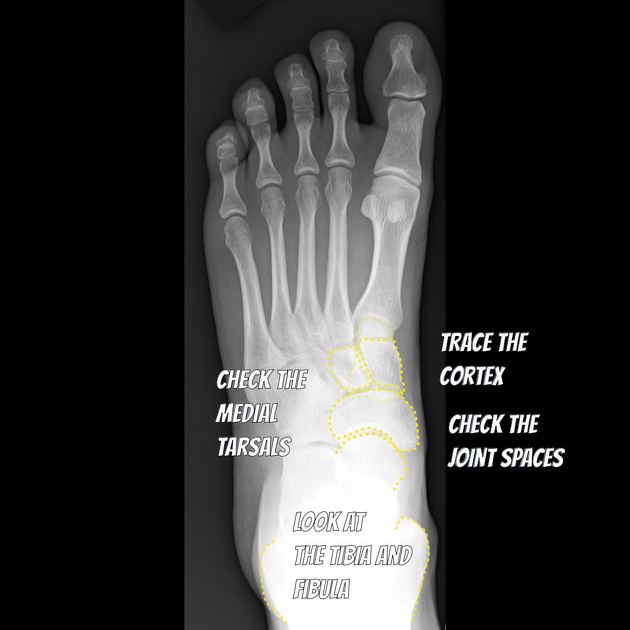
Bone review
-
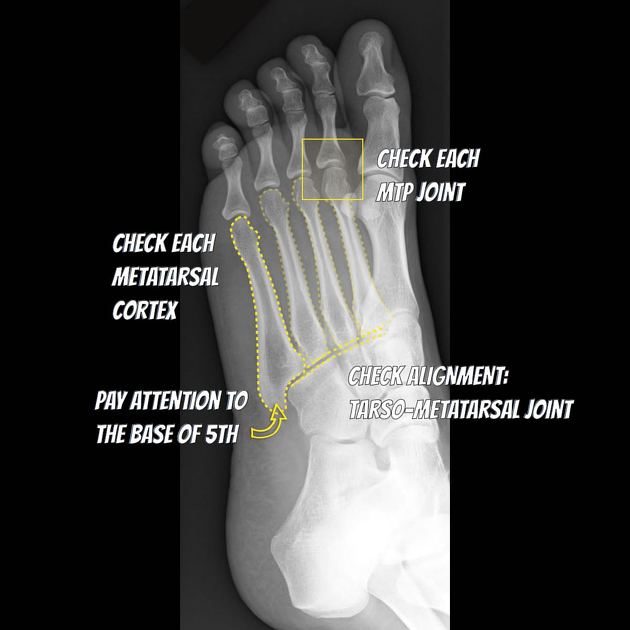
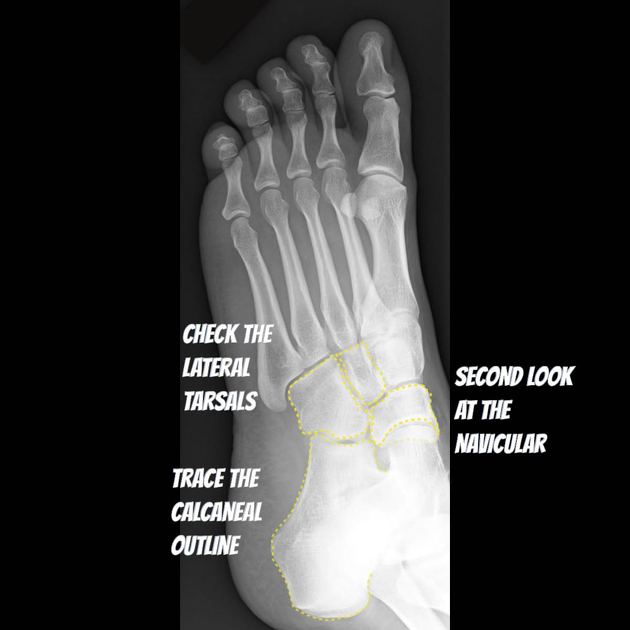
check around the cortex of every bone
start proximally and work distally, medial to lateral
check any tarsal coalition
-
look for any bone that is not attached
is it an ossicle, an avulsion or bone fragment?
do not call normal variant anatomy a fracture!
do not call an unfused base of 5th apophysis a fracture!
Alignment
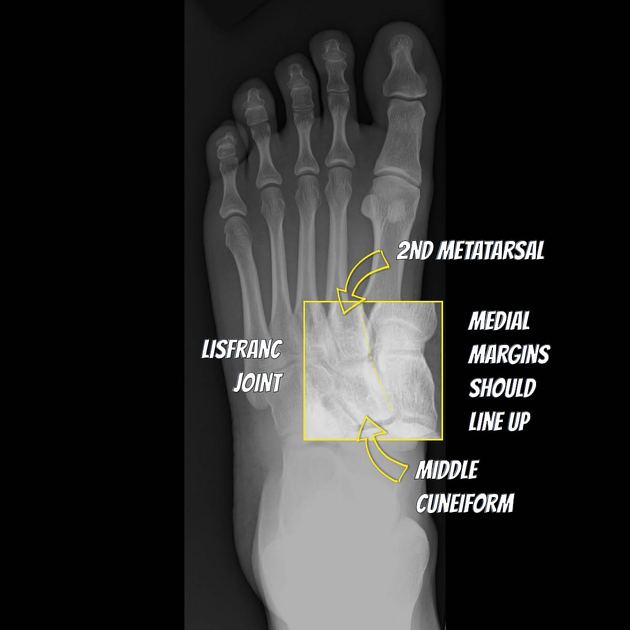
Lisfranc complex
The Lisfranc joint is hugely important for stability. Injury to it may be subtle and if missed, disastrous.
medial borders of 2nd metatarsal and intermediate cuneiform should line up on the DP (dorsiplantar) view
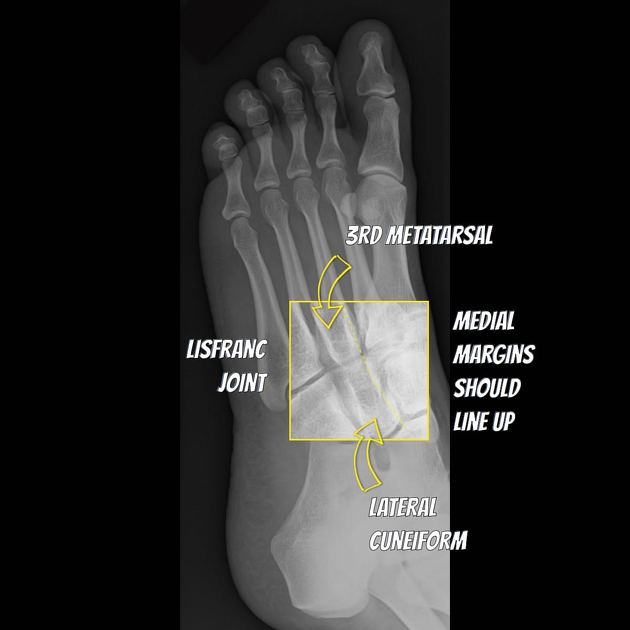
medial borders of 3rd metatarsal and lateral cuneiform should line up on the oblique view
if there is any step in either line, think Lisfranc injury
Medial aspect (DP)
1st and 2nd metatarsals
medial and intermediate cuneiform
Lateral aspect (oblique)
3rd, 4th and 5th metatarsals
lateral cuneiform
navicular and cuboid
Common pathology
Lisfranc injury
Lisfranc ligament between 1st and 2nd metatarsal bases
the ligament stabilizes the foot
widening of the 1st/2nd metatarsal space
a line along the medial margins of the 2nd metatarsal and intermediate cuneiform will be irregular
disruption suggests a huge injury
usually a crush injury or axial load to a plantarflexed foot
more: Lisfranc injury
Chopart injury
fracture / dislocation of the mid-tarsal joint (Chopart joint) of the foot, i.e. talonavicular and calcaneocuboid joints
foot is usually dislocated medially and superiorly as it is plantar flexed and inverted, usually as a result of high energy impact
more: Chopart fracture
Avulsion fractures associated with ankle sprain
Avulsion of the 5th metatarsal styloid
90% of base of 5th metatarsal fractures
avulsion of peroneus brevis tendon
forced inversion of plantarflexed foot (tennis fracture)
transverse fracture through tuberosity extending to tarsometatarsal joint
excellent prognosis
Dorsal capsular avulsion
curvilinear calcification dorsal to talar head or navicular bone
Extensor digitorum brevis avulsion fracture
thin calcification adjacent to anterolateral calcaneus on oblique view
Snowboarder's fracture
Jones fracture
base of 5th metatarsal fracture
transverse fracture 1.5-2 cm from tip of proximal tuberosity
forced inversion of plantarflexed foot
transverse fracture through diaphysis
high risk of nonunion
more: Jones fracture
Calcaneal fracture
extra-articular lover fracture (or Casanova fracture)
intra-articular lover fracture
calcaneal stress fracture
Do not miss
Stress fracture
commonly affect 2nd and 3rd metatarsal shafts
abnormal stresses lead to microfractures, e.g. marching
look for transverse fracture, periosteal reaction or callus













 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.