
Internal carotid artery (ICA) dissection, like arterial dissection elsewhere, is a result of blood entering the media through a tear in the intima 1 and is a common cause of stroke in younger patients.
On this page:
Epidemiology
Dissection may occur at any age but is a common cause of stroke in young patients 3,6. Internal carotid artery dissection has a prevalence of 20-25% of strokes in patients less than 45 years of age 3,6 and an annual incidence rate of 2.6 to 2.9 per 100 000 15. Cranio-cervical arterial dissections (including vertebral artery dissections) have an estimated incidence up to 5 cases per 100,000 in the general population 9. The mean age of occurrence is 45 years and there is a slight male predilection of ~55% 15. Curiously, there is a seasonal association with dissection more likely to occur in winter 6,29.
Risk factors
hypertension 16
migraine with aura 17-19
hyperhomocysteinemia 20-22
connective tissue disorder, e.g. Ehlers-Danlos syndrome, Marfan syndrome, osteogenesis imperfecta, fibromuscular dysplasia 23-25
cervical trauma 26
Clinical presentation
The classical presentation includes 6:
local pain
ipsilateral headache
ipsilateral neck pain
ipsilateral Horner syndrome
retinal ischemia
Unfortunately, this constellation of symptoms and signs is found in less than one-third of patients. Due to a lack of specific signs, the diagnosis often goes unrecognised for some time 6.
Pathology
Extracranial internal carotid artery dissection is more common than intracranial internal carotid artery dissection. It typically occurs 2-3 cm superior to the common carotid bifurcation and accounts for 2.5% of all first strokes 6.
Arterial dissection results from a tear in the tunica intima or vasa vasorum causing blood to enter the tunica media resulting in separation of the vessel wall and creation of a false lumen 16. Hematoma expansion towards the tunica adventitia can cause subadventitial dissection and may be accompanied by dissecting pseudoaneurysm or towards the intima resulting in subintimal dissection.
The internal carotid arteries, like the vertebral arteries, have a differing distribution of elastic fibers compared to similar sized vessels elsewhere (although this is disputed 12). Although the tunica media and tunica adventitia are present, they are only a third as thick as their extracranial counterparts, with the vast majority of elastic fibers located in a subendothelial elastic lamina. This fundamental difference accounts for the markedly different natural history of intracranial arterial dissections compared to their extracranial counterparts. When a tear breaches the aforementioned subendothelial elastic layer, then there is little tissue preventing extension into the subarachnoid space, thus accounting for the very high rate of subarachnoid hemorrhage.
Etiology
Causes of dissection can be separated into spontaneous, traumatic and iatrogenic 3:
-
spontaneous
especially in patients with fibromuscular dysplasia or connective tissue disorders, e.g. Marfan syndrome
-
traumatic
motor vehicle accidents, sport-related, strong coughing or nose blowing, chiropractic manipulation, lengthy telephone conversations 4,6
iatrogenic, e.g. cerebral angiography
Radiographic features
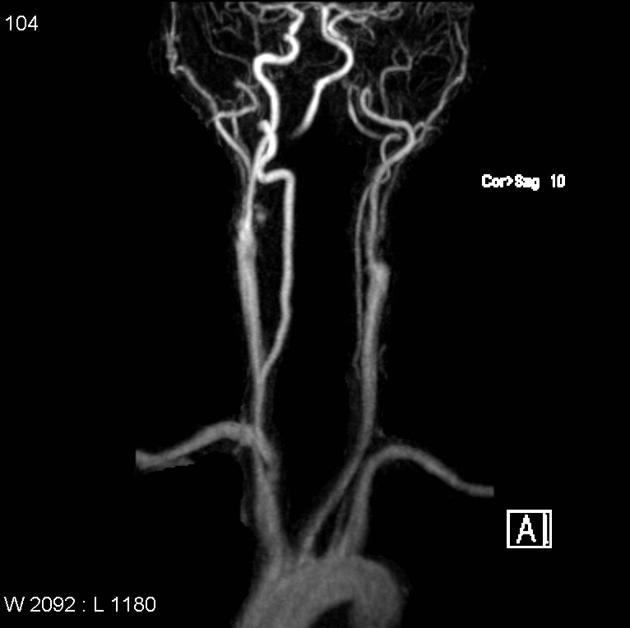
Spontaneous extracranial internal carotid artery dissection commonly originate near the level of the skull base and involves the distal portion of the cervical segment 14.
Ultrasound
Largely limited to the cervical portion of the carotid artery where flow aberrations, intramural hematoma, luminal thrombus and mobile flaps can be visualized. May present with double lumen sign. An eccentric echogenic component may be noted if an intramural hematoma is present 27.
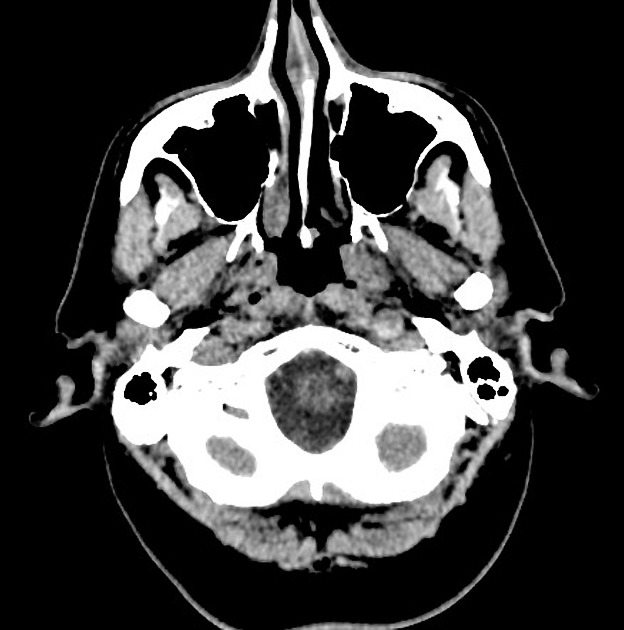
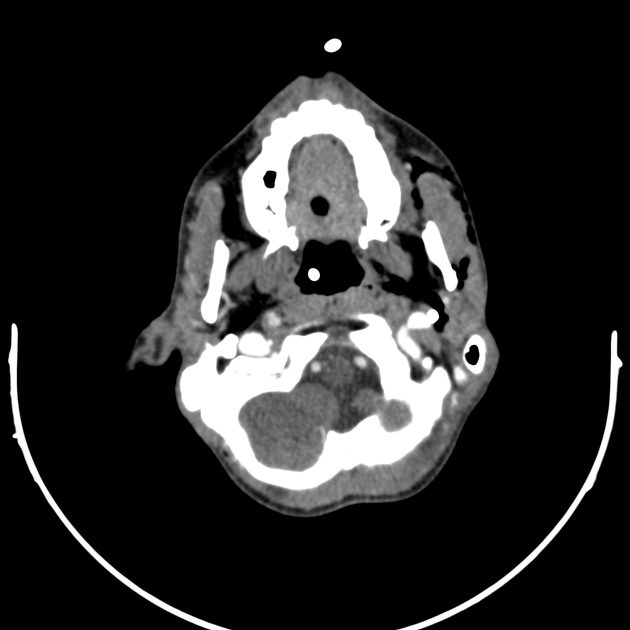
CT
-
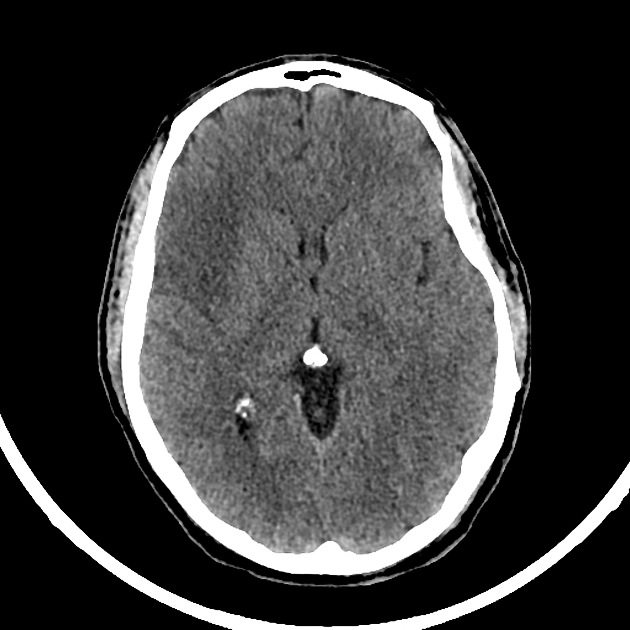
non-contrast brain CT is insensitive for dissection but may demonstrate
cerebral ischemia/infarct
arterial wall hematoma in the upper portion of the ICA as a spontaneous crescent-shaped hyperattenuating focus 9
-
CTA may demonstrate 7,9
enlargement of the dissected artery
an abnormal vessel contour (see DSA below): generally considered highly specific and sensitive
classical appearance: narrowed eccentric lumen surrounded by a crescent-shaped mural thrombus and thin annular enhancement (vasa vasorum enhancement in the adventitia)
intimal flap
dissecting aneurysm (internal carotid artery pseudoaneurysm)
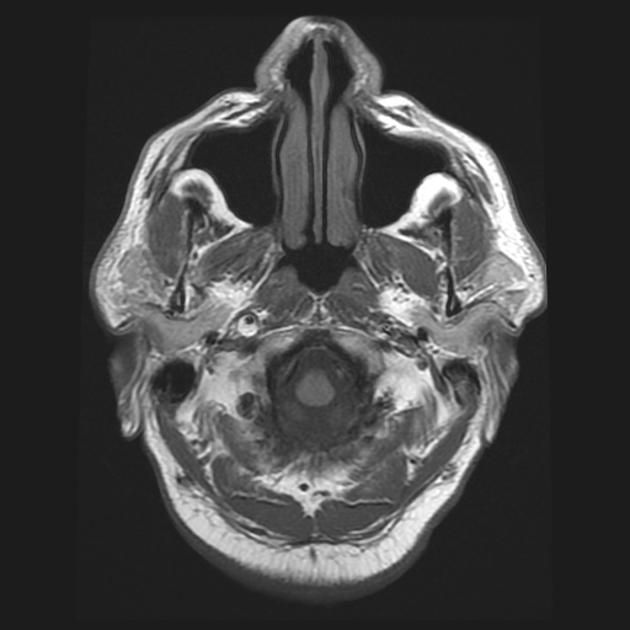
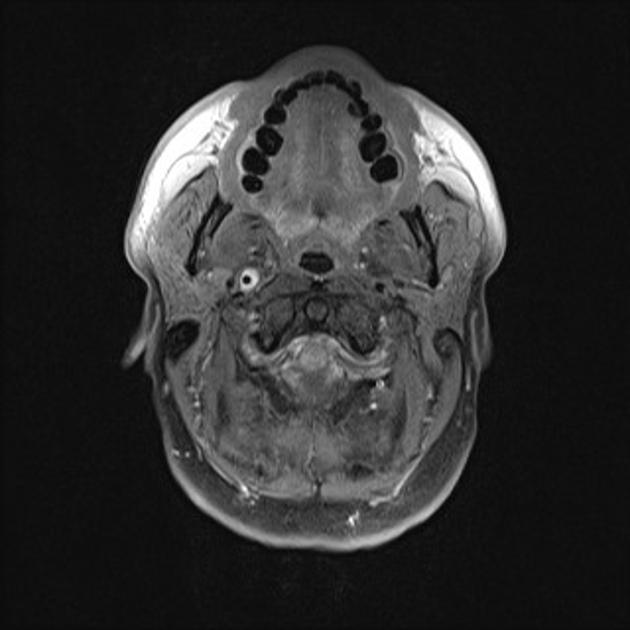
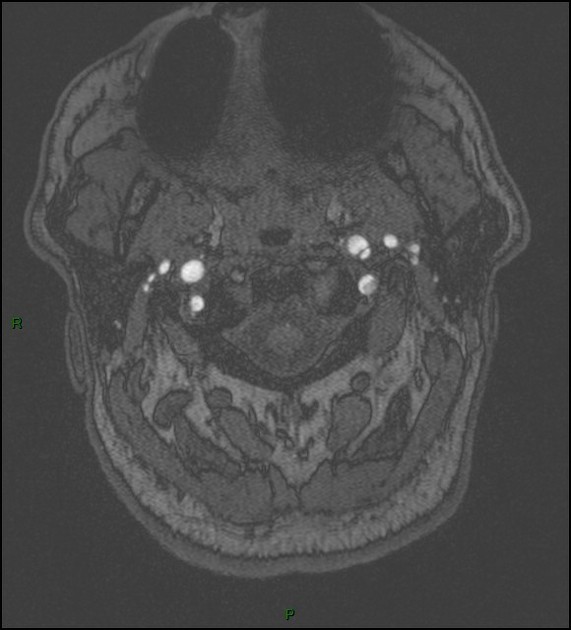
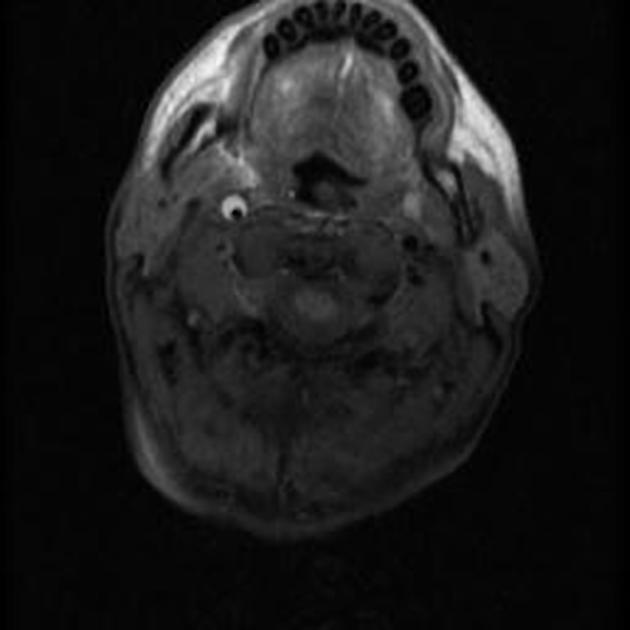
MRI
When cervical internal carotid artery is clinically suspected (such as in cases of carotid territory ischemia or neck trauma), the appropriate MRI protocol includes MRA of the neck to evaluate the lumen and axial fat-suppressed T1-weighted images (T1 FS) to evaluate for (subacute) intramural hematoma. However, when dissection is not suspected and the MRI protocol is not tailored accordingly, subpetrous internal carotid artery dissection with intramural hematoma can usually still be detected on routine brain MRI sequences including DWI 30.
MR interpretation of ICA dissection consists of two basic components:
-
primary detection of ICA dissection
T1 FS, T2, and DWI: high signal crescent sign indicating intramural hematoma
DWI: high signal crescent or circular indicating intramural hematoma
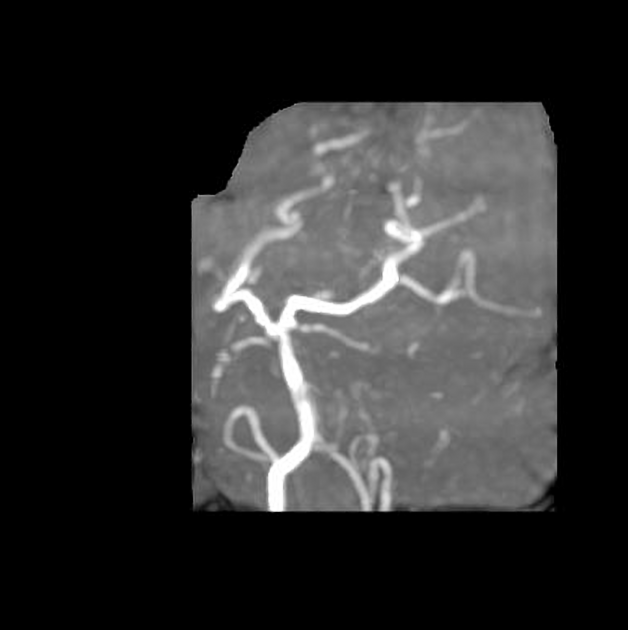
MRA: absent flow void or abnormal vessel contour
SWI: intramural hematoma 28
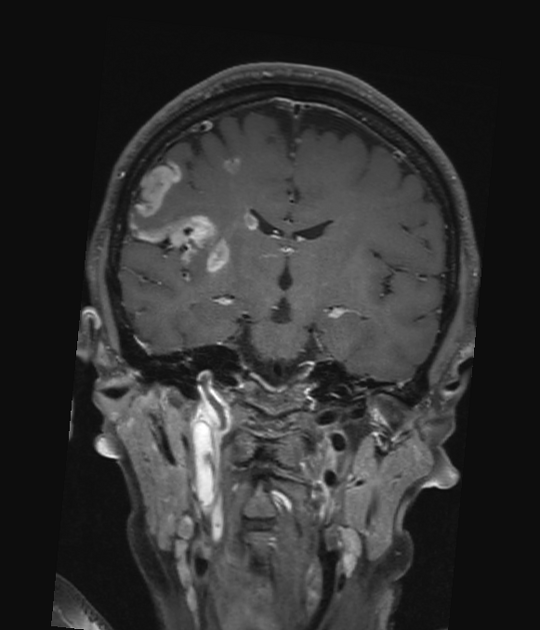
detection of secondary cerebral infarction on DWI/ADC and FLAIR
Angiography (DSA)
Although considered the gold standard, digital subtraction angiography does not always demonstrate definite signs of ICA dissections as the thickness and contents of the arterial wall may not be clearly demonstrated 9. The following may be evident:
vessel wall irregularities
string and pearl sign: focal narrowing with a distal site of dilatation
pseudoaneurysm formation: see internal carotid artery pseudoaneurysm
double barrel lumen or intimal flap are rarely seen 2,9
Treatment and prognosis
Conservative medical management is often all that is required. This consists of antiplatelet therapy, with or without anticoagulation 3. If the patient is symptomatic and there are ongoing ischemic events that are not controlled by medical management, endovascular treatment may be of benefit. Endovascular options include gentle angioplasty and stent placement 3.
Surgical intervention has a limited role in modern practice and usually consists of bypass or ligation. Detailed knowledge of the circle of Willis anatomy is essential when assessing collateral pathways.
Differential diagnosis
-
ICA bilateral involvement reported in ~65% 9
multifocal stenosis with adjacent dilatations also referred to as the string of beads sign
-
involves the carotid bulb
ulcerated plaque may mimic an intimal flap on axial images
dysgenesis of the ICA: carotid canal is absent or hypoplastic
isolated traumatic ICA pseudoaneurysm: may be indistinguishable from a dissection pseudoaneurysm








 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.