
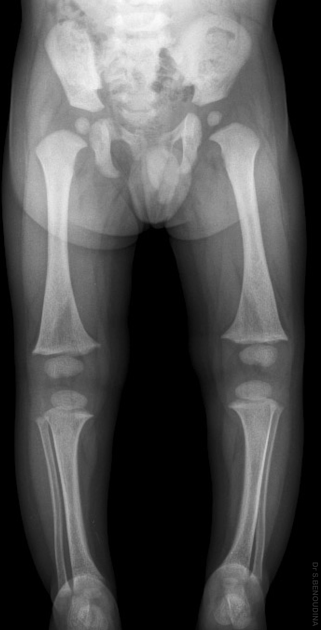
Leg bowing in children is common and often developmental.
Differential diagnosis
The differential includes:
- developmental bowing
- exaggeration of normal age-related angulation changes at the knee
- neonates and infants normally have varus angulation that gradually corrects within 6 months of walking or by 2 years of age
- changes to valgus angulation at age 2-3 years and reverts to the adult pattern by age 6-7 years
- more common if begin walking at an early age, heavier children, and African-American children
- does not require treatment, but should follow-up to ensure resolution of bowing and ensure that tibia vara does not develop
- congenital bowing
- secondary to abnormal intrauterine position
- localized skeletal dysplasia or fetal vascular insufficiency may play a role in some cases
- usually bowing of tibia/fibula convex posteriorly and medially, less commonly convex laterally
- good prognosis for remodeling during growth, but bracing may be necessary in some cases
- associated leg-length discrepancy is usually seen
- secondary to abnormal intrauterine position
- rickets
- scurvy
-
Blount disease
- tibia vara
- metaphyseal-diaphyseal angle >11° (in contrast to <8° in developmental bowing)
- usually unilateral or asymmetric (in contrast to symmetry of developmental bowing)
- focal fibrocartilaginous dysplasia
-
neurofibromatosis type 1
- usually anterolateral bowing of the tibia with or without a hypoplastic fibula
- skeletal dysplasias
- osteomyelitis
- syphilis: sabre shin
- yaws: boomerang tibia





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.