
Pellegrini-Stieda lesions are ossified post-traumatic lesions adjacent to the margin of the medial femoral condyle.
On this page:
Clinical presentation
Most patients are asymptomatic, while a small proportion will have medial knee pain (Pellegrini-Stieda syndrome) 7.
Pathology
Pelligrini Stieda lesions likely represent a range of traumatic lesions, with possible origins including:
-
medial collateral ligament (MCL)
avulsion fracture of the superficial MCL attachment at the medial femoral condyle (Stieda fracture) 5,7
deep MCL 6
adductor magnus muscle ischiocondylar insertion 2,5
medial femoral condyle periosteal stripping 2
medial patellofemoral ligament insertion 6
Calcification/ossification usually begins to form 3-4 weeks after the initial injury 5.
Associations
Radiographic features
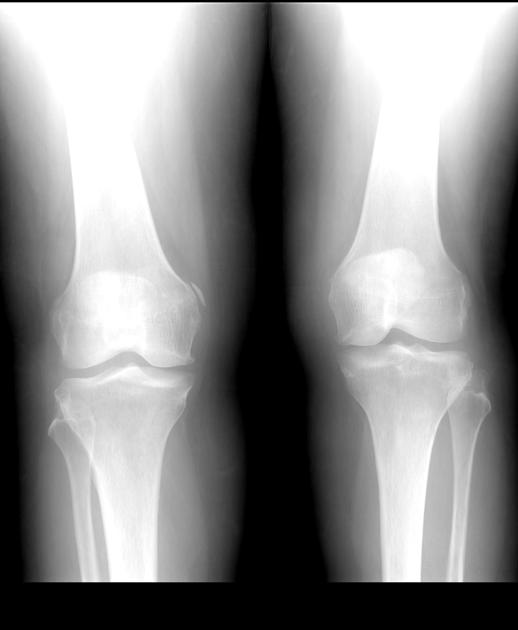
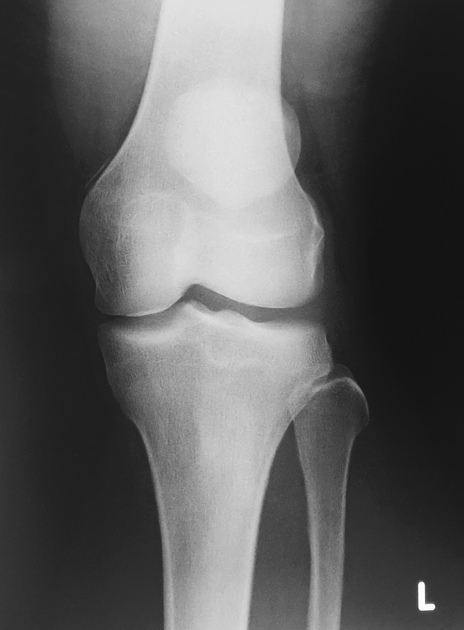
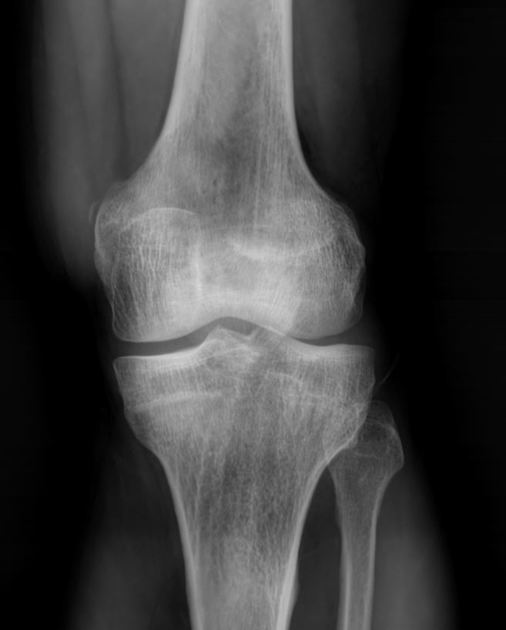
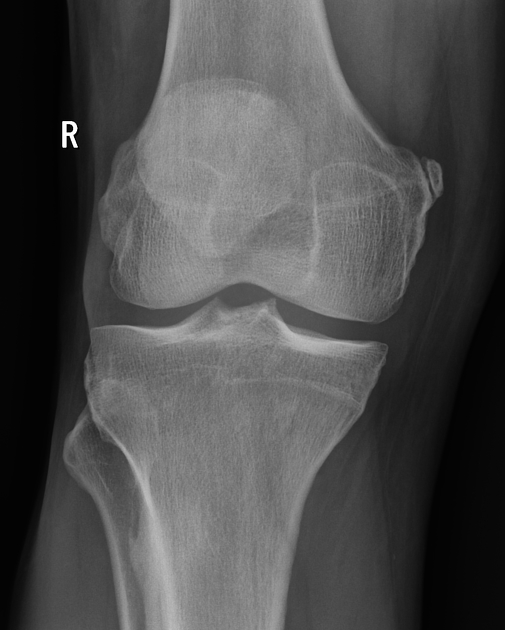
Plain radiograph
Calcification/ossicles or enthesophytes adjacent to or above the medial femoral condyle, which is often linear or curvilinear in shape and parallels the femoral cortex 5.
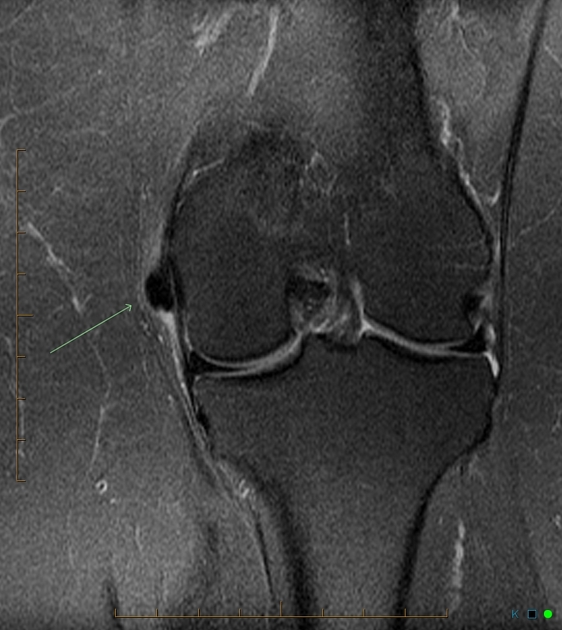
MRI
Pellegrini-Stieda lesion as an ossicle or enthesophyte showing a bone marrow signal at or above the medial femoral condyle. The medial collateral ligament is usually thickened.
Treatment and prognosis
Mild and moderate cases (i.e. Pellegrini-Stieda syndrome) are often conservatively managed 6 with steroid injections and range-of-motion exercises. Surgical excision of calcifications and medial collateral ligament repair is considered mainly for refractory cases 3,6.
History and etymology
This lesion was first described by German radioloist, Alban Köhler (1847–1947) in 1903 7. However, it is named after Italian surgeon, Augusto Pellegrini (1877-1958), who stated the calcifications were at the origin of the MCL in 1905, and German surgeon, Alfred Stieda (1869-1945), who reported a case series in 1908 7.
Differential diagnosis
tendinous calcification in reactive arthritis: often exhibits other degenerative changes

















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.