
Pes planus (plural: pedes plani) is a deformity of the foot where the longitudinal arch of the foot is abnormally flattened and can be congenital or acquired.
On this page:
Terminology
Pes planus is also known as flatfoot, planovalgus foot or fallen arches 7.
Epidemiology
Pes planus may occur in up to 20% of the adult population, although the majority of patients are asymptomatic and require no treatment. Approximately 10% (range 7-15%) of the population with developmental flatfoot go on to develop symptoms requiring medical attention 7.
Associations
There are several conditions associated with pes planus 1,2:
-
certain connective tissue disorders
There is some evidence to suggest that flat feet increases the risk of stress fractures 10.
Pathology
Pes planus can be 7:
congenital: normal in toddlers, may persist into adulthood
-
acquired secondary to:
posterior tibialis dysfunction (most common) 4
trauma
neuromuscular disease
In the pediatric population, the degree of ligamentous laxity of the foot results in relative pes planus that resolves over time 5. Within the first decade, there is spontaneous development of a strong arch in most people 7.
Pes planus results from loss of the medial longitudinal arch and can be either rigid or flexible. These deformities are usually flexible, which means that on non-weight-bearing views, the alignment of the plantar arch normalizes.
Radiographic features
Plain radiograph
The longitudinal arch of the foot must be assessed on a weight-bearing lateral foot radiograph. If the patient is unable to stand or weight-bear, a simulated weight-bearing radiograph should be obtained.
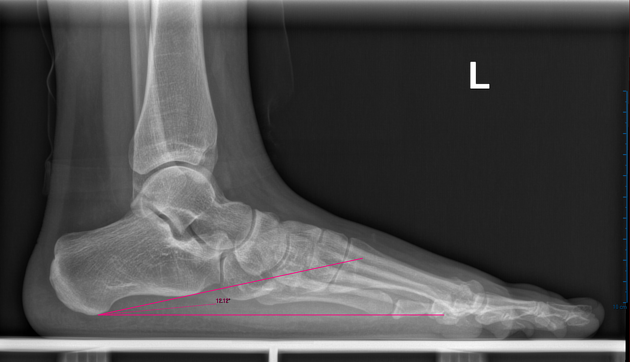
Weight-bearing lateral view
In normal feet, the relationship between the talus and the 1st metatarsal results in a straight line being formed along their axes (i.e. normal Meary's angle = 0°). Pes planus, in contrast, will show 7:
loss of the normal straight-line relationship with Meary's angle >4° convex downwards
sagging at the talonavicular or naviculocuneiform joints
calcaneal inclination angle ≤19° 9
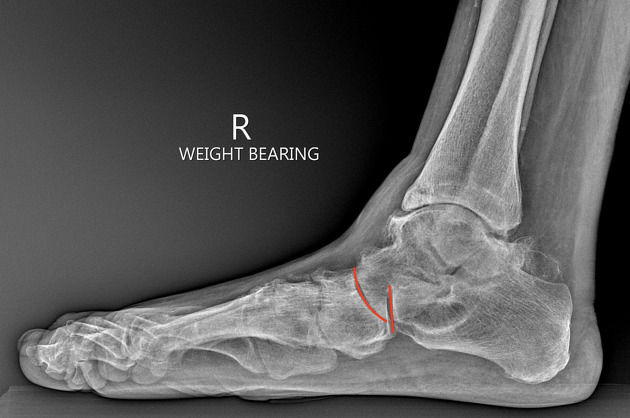
disruption of the cyma line: appears as a "lazy S-shape" of the talonavicular and calcaneocuboid joints on both AP and lateral views; it is disrupted owing to anterior shift of the talonavicular joint 8
Weight-bearing dorsoplantar view
It is important to assess:
hindfoot valgus (where the talocalcaneal angle is >35°)
talonavicular undercoverage or subluxation (where the talonavicular coverage angle is >7°)
forefoot abduction
Congenital vs acquired
Acquired pes planus (i.e. foot collapse) can be distinguished from congenital pes planus by carefully assessing the calcaneus and midtarsal joint: 6
in the acquired form, the calcaneal pitch is at least 10°; in congenital pes planus it is less
in the acquired form, the calcaneus is downwards-concave; in the congenital form it is downwards-convex or flat
in the acquired form, the midtarsal joint is altered by a forward-jutting talus; in the congenital form the talus is medially displaced, but the midtalar line appears normal (i.e. it is pseudonormal)
Treatment and prognosis
Treatment depends on whether:
there are symptoms
it is fixed or mobile
there are associated findings, e.g. hindfoot valgus
there is any associated pathology
Subtalar arthroereisis can be performed in pediatric symptomatic flexible flatfoot. In fixed flatfoot, non-operative management is unlikely to be beneficial since there is a fixed relationship between osseous structures.










 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}