
Tarlov cysts, also called perineural cysts, are CSF-filled dilatations of the nerve root sheath at the dorsal root ganglion (posterior nerve root sheath). These are type II spinal meningeal cysts that are, by definition, extradural but contain neural tissue.
Most Tarlov cysts are asymptomatic, but in some individuals can lead to neurological dysfunction and pain. These have been termed sacral symptomatic Tarlov cysts 6.
On this page:
Epidemiology
Tarlov cysts are common and are found in up to 4.6% of the population, more commonly in women 9.
Associations
They have occasionally been associated with connective tissue disorders:
Clinical presentation
The prevalence and severity of symptoms in patients with Tarlov cysts are controversial. Traditionally, and still largely the dominant view, it has been believed that like other spinal meningeal cysts, the vast majority of Tarlov cysts are incidentally found and are entirely asymptomatic. Large cysts may cause local pressure effects and remodel bones. However, symptoms don't appear to correlate well with size 2.
In some patients, however, it appears that Tarlov cysts are the cause of symptoms, such as pelvic or perineal pain/discomfort, sphincter/sexual dysfunction, radicular pain/numbness, and neurogenic claudication 3,6.
Radiographic features
Whilst Tarlov cysts are most common in the lower lumbar spine and the sacrum, they can occur anywhere in the spine.
Tarlov cysts appear as very thin-walled CSF intensity simple cystic structures closely related to sacral and lower lumbar nerves. The sacral foramina may be widened. Morphology can vary from a simple rounded cyst to a complex loculated cystic mass with septations.
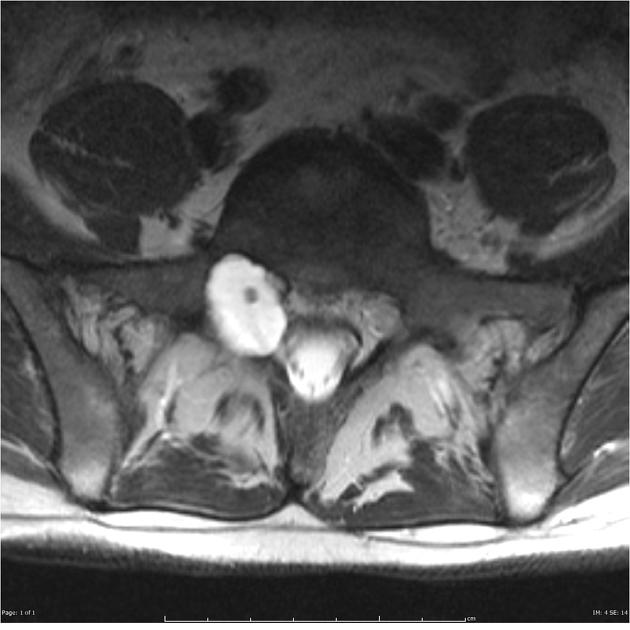
MRI
On MR the perineural cysts predominantly originating near the sacral nerves adjacent to the dorsal root ganglion. Signal characteristics of typical Tarlov cyst are those of CSF on all sequences.
T1: low signal
-
T2:
high signal 9
will show chemical shift at fat-fluid boundary with epidural fat
T1 C+: no enhancement
DWI/ADC: facilitated diffusion ~3000 x 10-6 mm2/s
Treatment and prognosis
In asymptomatic individuals no treatment or further investigation is necessary. This accounts for the vast majority of Tarlov cysts.
In patients with otherwise unexplained neurological symptoms potentially attributable to the cysts then further investigation and/or treatment may be warranted.
Electromyography can be used to identify axonal damage in symptomatic patients 6.
Cysts thought to be symptomatic can be aspirated under CT guidance using a two-needle technique and fibrin can be injected as a sealant 7.
Numerous surgical approaches have also been described 7.
History and etymology
Tarlov cysts were initially described by the American neurosurgeon Isadore Max Tarlov (1905-1977) in 1938 1,6,8.
Differential diagnosis
Usually, the diagnosis is self-evident and no alternatives should be entertained. Occasionally appearances are atypical and possible differential considerations include:

















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.