
Tendinopathy has been defined as "persistent tendon pain and loss of function related to mechanical loading" 7 but is also used as a broad term used to describe any problem involving a tendon.
On this page:
Epidemiology
The prevalence of tendinopathy in the general population is 2-5%. Active and sporting individuals are at increased risk of tendinopathy although it is also commonly seen in non-active individuals. The prevalence in some populations can be high, e.g. patellar tendinopathy in up to 40% of volleyball players, however, sites and prevalence will depend on the sport and level played 2.
Risk factors
Risk factors can be intrinsic or extrinsic 2,7:
-
intrinsic
genetic: strongest association with COL5A1, TNC, MMP3 and ESRRA
sex: increased in female
age: increases with age
medications, e.g. fluoroquinolones, local and systemic glucocorticoids
metabolic, e.g. obesity, type 2 diabetes mellitus, dyslipidemia, hypercholesterolemia
poor muscle strength
-
extrinsic
excessive tendon beyond tendon capacity, in particular, activities with a high-energy storage component (e.g. jumping in basketball, kicking sports)
amount of loading (e.g. increased training time, overuse)
change in loading
"abusive loading" (i.e. unaccustomed activity) in non-active individuals
impingement
occupations with high force and/or repetitive activities, e.g. hospitality, factory work, construction, surgeons
Clinical presentation
Tendinopathy is a clinical syndrome consisting of pain, tenderness, tendon swelling and impaired function 3.
Pathology
The pathophysiology of tendinopathy is yet to be fully elucidated but one popular theory is the continuum model with inflammation rather than degeneration implicated 2,3:
reactive tendinopathy
tendon dysrepair (also known as "failed healing")
degenerative tendinopathy
Others include mechanical, inflammatory, apoptosis, and vascular/neurogenic theories 7.
Tenocyte proliferation occurs with adaptive chondrometaplasia. Mucin deposition in connective tissues, fiber disruption of collagen and vascular proliferation. Deposition of fat or calcification may occur.
Location
Tendinopathy most commonly occurs in the 7:
-
upper limb
shoulder: supraspinatus tendinopathy
elbow: common extensor and common flexor tendinopathy
-
lower limb
Other locations include
Radiographic features
Ultrasound is the mainstay of imaging tendinopathy, with MRI as the second-line investigation. Plain radiograph and CT have a limited role, sometimes used to assess for calcification or associated avulsion injuries.
Plain radiograph
Plain radiographs have a low sensitivity for tendinopathy but localized soft tissue swelling and calcifications/ossification may be seen. Calcified insertional tendinopathy is usually well seen and is a common incidental finding.
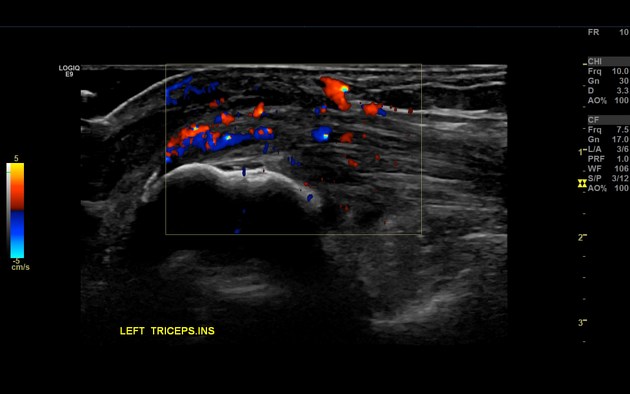
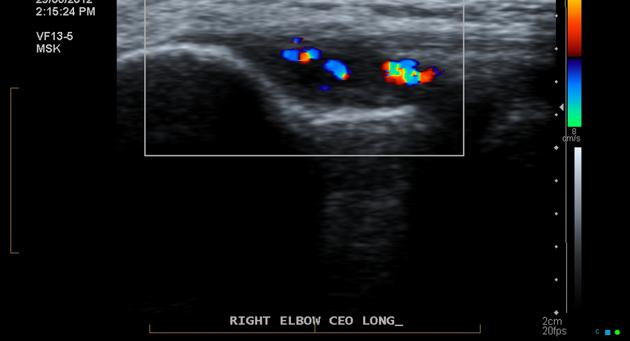
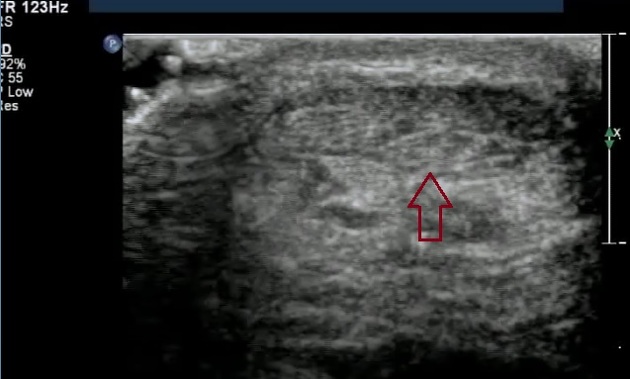
Ultrasound
Specific features will depend on the site of tendinopathy but general features include 4:
early changes: tendon thickening, contour change, echotexture change
progressive changes: further tendon thickening, loss of normal fibrillar pattern with hypoechoic heterogeneity
may be focal or diffuse
color Doppler may demonstrate neovascularity
The above changes can be seen in asymptomatic individuals but prominent, tendon thickening, loss of fibrillary pattern and neovascularity are more commonly seen in symptomatic patients 4.
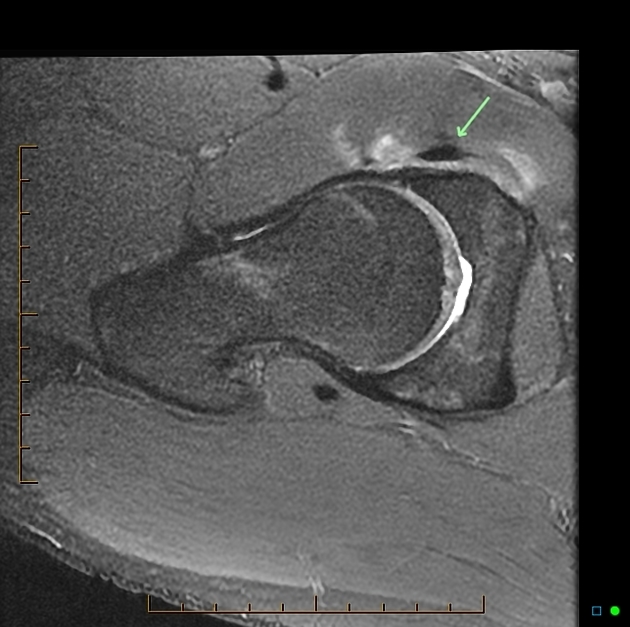
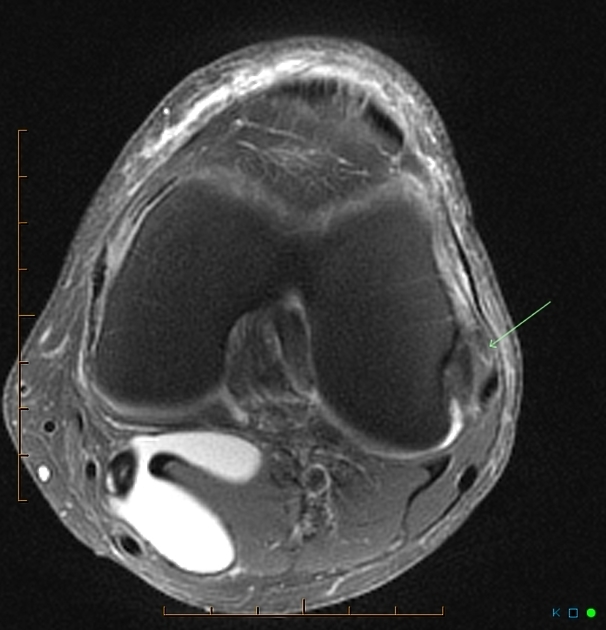
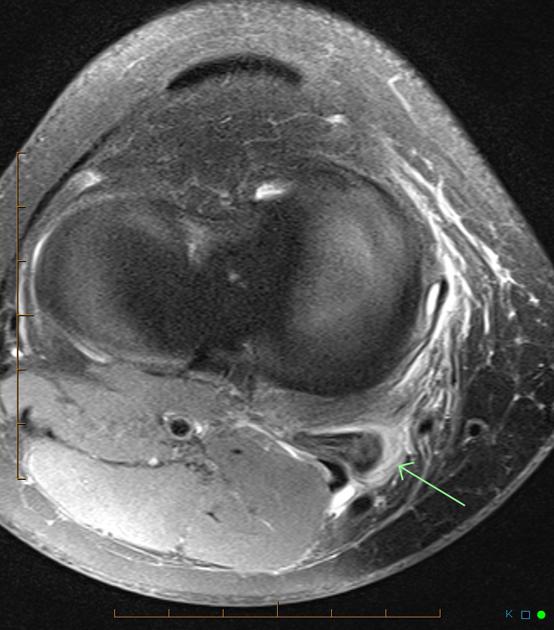
MRI
There is overlap in the imaging features on ultrasound with tendon thickening and contour change present 5.
T1: hyperintense
T2: hyperintense
GRE: hyperintense (often before T1 spin-echo hyperintensity) 5
T1 C+ (Gd): enhancement 5
Unfortunately, these features are indistinguishable from myxoid degeneration.
Chronic insertional tendinopathy may demonstrate a tear with adjacent bony proliferation at the tendon insertion, with our without marrow edema.
Differential diagnosis
adjacent capsular or ligamentous injuries
on ultrasound, anisotropy artifact can mimic hypoechoic tendinopathic changes 4
on MRI, magic angle artifact can mimic hyperintense tendinopathic changes 5


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.