
Presentation
Acute epigastric pain. Not known to have gastric or duodenal ulcer.
Patient Data
Note: This case has been tagged as "legacy" as it no longer meets image preparation and/or other case publication guidelines.
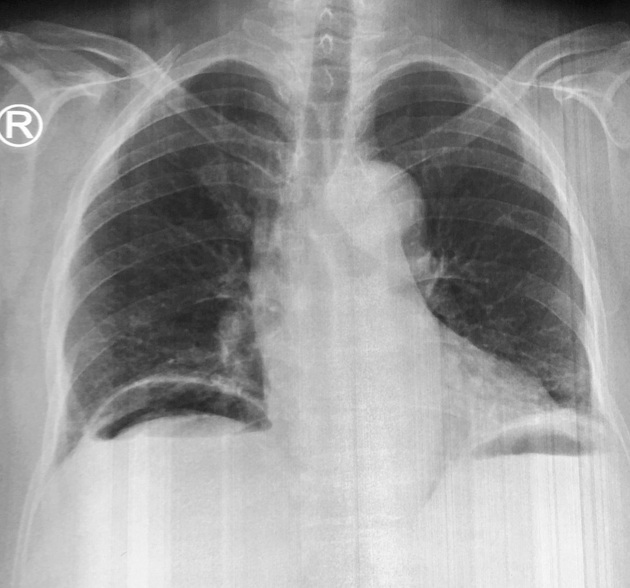
Moderate amount of subdiaphragmatic air on the right side.


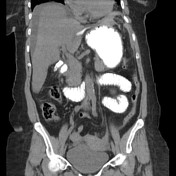

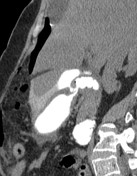
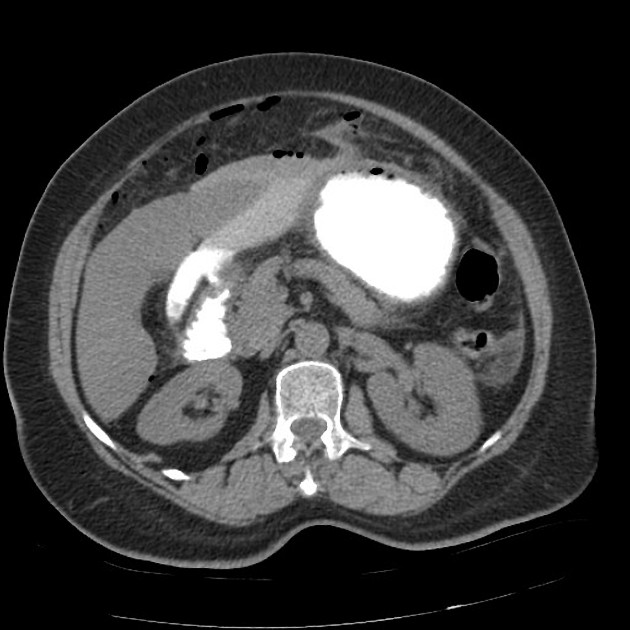
CT after oral contrast shows a thickened duodenal wall involving the first part of the duodenum, with an evident defect through which the oral contrast material leaks into the peritoneal cavity, including into the peri- and subhepatic regions. There is also pneumoperitoneum. Signs of peritoneal irritation can be seen also in the form of stranding of the central mesenteric fat with some jejunal wall edema.
Case Discussion
A straightforward case of bowel perforation with typical clinical presentation and confirmatory pneumoperitoneum on standing plain x-ray. The exact site of perforation was nicely demonstrated on CT study with oral contrast, with leakage of oral contrast into the peritoneal space at the first part of the duodenum.
Gastric and duodenal ulcers usually have similar risk factors and both can be complicated by perforation, however they may vary a little bit in their clinical presentation.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.