
Presentation
Known patient of Crohn disease came with increasing abdominal pain.
Patient Data
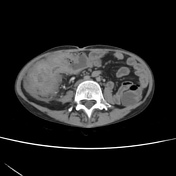


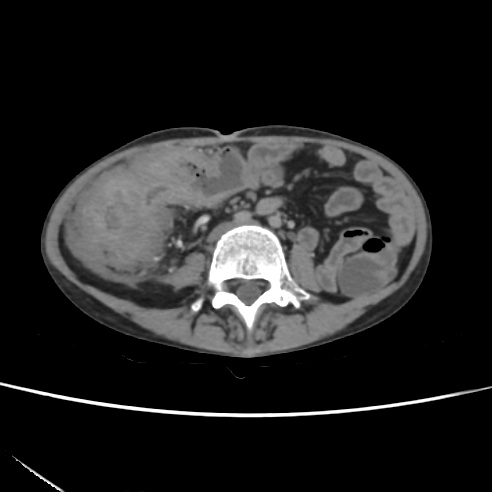
Pulled up cecum. Extensive circumferential mural thickening and stratification is seen involving cecum, ascending colon, and proximal third of transverse colon with a colocolic fistulous track communicating between ascending colon and transverse colon. There is extensive pericolonic fat stranding surrounded by multiple enlarged inflamed lymph nodes. Engorged vasa rectae with mild fluid in paracolic gutter.
Rest of the bowel loops are normal. All other solid abdominal viscera are normal.
Case Discussion
Episodes of exacerbation and remission are commonly encountered in inflammatory bowel disease.
Some of the long term commonly encountered complications include bowel strictures, adhesions, enterocutaneous or enteroenteric fistulations, intra abdominal abscess formation.
The prior study of this patient done 5 months ago (images not provided) did show the extensive large bowel involvement, however no fistulation existed. This is a new development. No intra-abdominal abscesses are present though.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.