
Presentation
History of heart failure, presenting with vomiting and jaundice. Serum labs show bilirubin 13 mg/dL, alkaline phosphatase 250 IU/L, AST/ALT 200s IU/L.
Patient Data









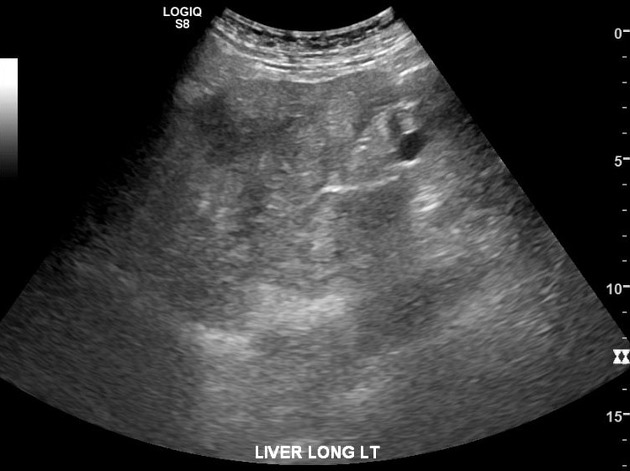
Heterogenous liver parenchyma, markedly hyperechoic relative to right kidney indicating steatosis. Posterior to the gallbladder, there is an ill-defined hepatic mass measuring ~6.6 cm, in the region of the caudate lobe.



Diffuse patchy parenchymal hypoattenuation in a nodular pattern, somewhat sparing the anterior liver. The caudate lobe is prominent, appears enlarged by masslike hypodensity. Notably, the hepatic vessels remain evident coursing through the areas of hypoattenuation.
Liver surface remains smooth along the anterior surface, although there are segments of nodularity along the inferior liver surfaces (e.g. along gallbladder fossa). Overall liver size appears mildly enlarged.

Representative image from random liver biopsy.
Random liver biopsy, right lobe
Microscopic description
Moderate large droplet macrovesicular steatosis, involving approximately 50% of hepatocytes (score 2). There is prominent ballooning degeneration with Mallory Denk bodies (score 2) and lobular inflammation (>4 foci/ 20x field; score 3), with satellitosis. Trichrome stain highlights marked pericellular fibrosis, with extensive bridging fibrosis (stage 3). There is focal 1-2+ reticuloendothelial iron deposition (iron stain). There are no diastase resistant cytoplasmic globules in hepatocytes (PASD stain). Reticulin stains on both blocks confirm absence of hepatocellular carcinoma. With prominent neutrophilic lobular inflammation, satellitosis and conspicuous Mallory Denk bodies, histologic features suggest alcoholic fatty liver disease.
Impression
Steatohepatitis, NAS score 7 of 8, fibrosis stage 3 (NASH-CRN system)

Representative images from CT-guided core needle biopsy of caudate lobe.
Liver, "caudate lesion"
Microscopic description
Sections of the liver biopsy show altered architecture. There is bridging fibrosis, evident on H&E stain, with vague nodularity. There is moderate macrovesicular, large droplet steatosis, involving approximately 50 to 60% of the liver parenchyma (grade 2). Ballooning hepatocytes is prominent (grade 2), with abundant poorly-formed Mallory-Denk bodies. Satellitosis is seen. Acidophil bodies are also noted. Lobular inflammation is diffusely present (severe, grade 3), composed of a mixed infiltrate of neutrophils, eosinophils, as well as lymphohistiocytic infiltrate. Canalicular cholestasis is present. Special stains are performed on section A1. Trichrome stain highlights complex perisinusoidal fibrosis with bridging fibrosis and focal nodule formation. The PAS stain with diastase highlights increased macrophages in the areas of lobular inflammation, but is negative for diastase resistant alpha-1 antitrypsin globules and hepatocytes. The iron stain is negative for hepatocellular iron accumulation, but highlights scattered, rare reticuloendothelial iron accumulation. The reticulin stain is not informative due to technical problems.
Impression
- Steatohepatitis (NAS score 7/8) and acute cholestasis
- Complex perisinusoidal and bridging fibrosis with focal nodule formation (Stage 3-4)
- No tumor identified
Case Discussion
This case exemplifies how tricky nodular steatosis can be.
Ultrasound findings of diffuse diffusely increased echogenicity, coarse echotexture, and heterogeneous parenchyma suggest steatosis. CT findings of patchy liver hypoattenuation which approaches the density of macroscopic fat also suggest profound steatosis; note how the hepatic vessels are stereotypically preserved as they course through the regions steatosis. In addition, faint nodularity along the liver undersurface hints at a degree of hepatic fibrosis.
The caudate lobe drew attention on both ultrasound and CT because it resembles a discrete mass, although in retrospect shares similar characteristics with adjacent steatotic liver. Patient initially underwent random liver biopsy to asses overall liver disease, and after further discussion went for biopsy of the caudate region to exclude malignancy.
Thanks to Dr. Kevin Liu.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.