
Presentation
Known case of right breast cancer on chemotherapy presented by dyspnea, cough, and respiratory failure.
Patient Data

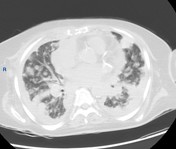
Multiple, variable-sized poorly defined heterogeneous opacities are seen scattered at both lung parenchymas.
Obliterated costophrenic angles bilaterally suggest pleural effusions.
Multiple scattered osseous lytic foci along ribs and both clavicles.



Right breast heterogeneous multiple soft tissue masses the largest measuring about 4.6x2.8 cm at right inner quadrant with speculations, small calcifications, and blurred fat planes, moreover enlarged suspicious axillary lymphadenopathy.
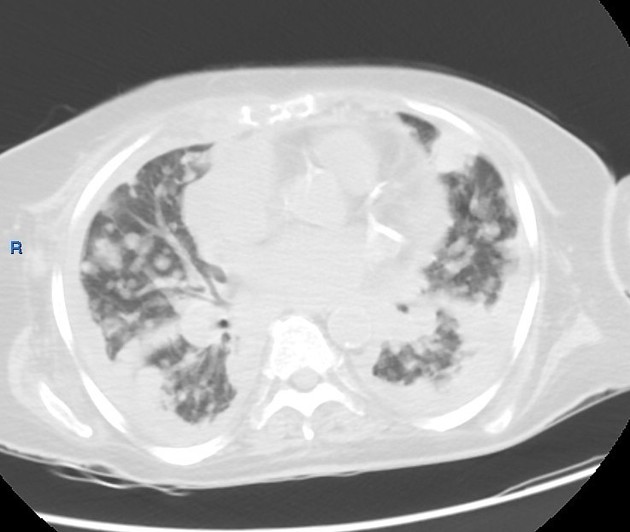
Both lung fields are studded with numerous (innumerable), variable size pulmonary nodules seen scattered at both lung fields giving the characteristic cannonball appearance of pulmonary deposits. Some of these nodules are pleural based and some conglomerate together forming large masses.
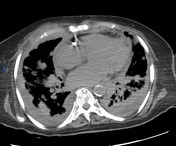
Mild bilateral basal pleural effusion/ collection.
Multiple scattered focal pleural thickening more along mediastinal and diaphragmatic surfaces.
Diffuse interstitial pulmonary reaction with peri-lymphatic nodules, thickening, thickened interlobar septae, reticulations, and reticulonodular infiltrates.
Slightly prominent mediastinal lymph nodes seen in the peri-vascular region at the thoracic inlet, internal mammary, aortopulmonary, paratracheal, aortocaval, and possible hilar groups.
Mild cardiomegaly.
Upper abdominal cuts right hepatic lobe focal lesion.
Multiple vertebral, sternal, ribs, and clavicular scattered osteolytic metastatic deposits.
Case Discussion
Findings are impressive of advanced metastatic breast cancer with lymphadenopathy, cannonball pulmonary metastases, pleural thickening, and pulmonary lymphangitic carcinomatosis as well as osseous metastatic deposits.
Breast cancer is an uncommon cause of cannonball metastasis of the lungs.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.