
Presentation
Persistent cough.
Patient Data


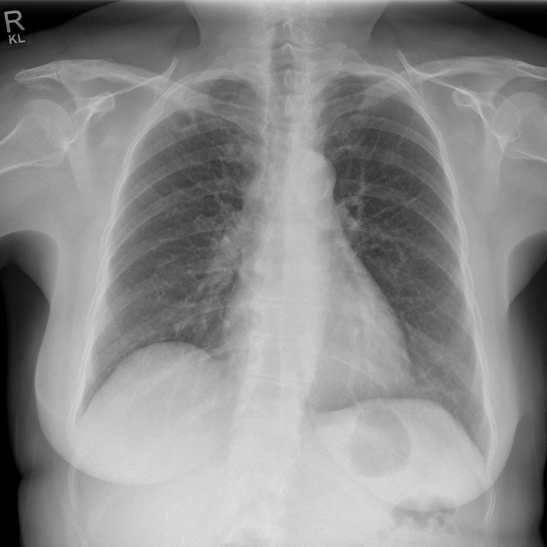
Approximately 2 cm diameter right upper lobe cavitating lesion, projecting between the anterior aspects of the right 1st and 2nd ribs.
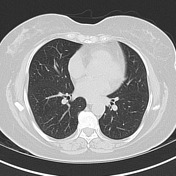


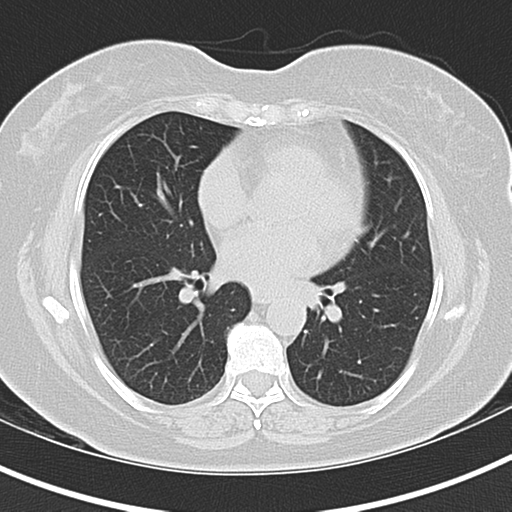
Dominant right upper lobe cavitating nodule. Several smaller nodules in the right lower lobe. No lymphadenopathy. No destructive bone lesion.

A lung lobectomy specimen 135 x 115 x 47 mm with bronchovascular remnants up to 13mm and a few black hilar lymph nodes are present up to 8 mm. Adjacent to the hilum there is a staple line 105mm in length. Pleura inked blue, staple line removed and resulting surface inked black. Opposite the hilum, 45 mm from bronchovascular margins and 55 mm from the stapled margin, there is a well demarcated firm white tumor with a central cavitation 25 x 19 x 12 mm. Tumor extensively abuts the pleura which is puckered and roughened. The remaining lung is unremarkable.
Case Discussion
The differential for a cavitating lesion most commonly includes malignancy and infection. This cavitating mass had grown between follow-up scans, had FDG avid walls on a PET-CT, and thus went for resection.
Cavitating malignancies include primary lung cancer (namely squamous cell carcinomas) and cavitating metastases, with the latter being the diagnosis in this case. Interestingly, histopathology demonstrated an endometrial primary of which the patient had a history of stage 2 endometrial carcinoma diagnosed three years earlier. Endometrial cancer is not on the usual list for causes of cavitating pulmonary metastases.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.