
Presentation
Abdominal pain. Large, palpable abdominal mass with visible abdominal distention.
Patient Data
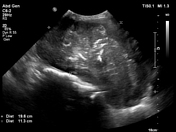

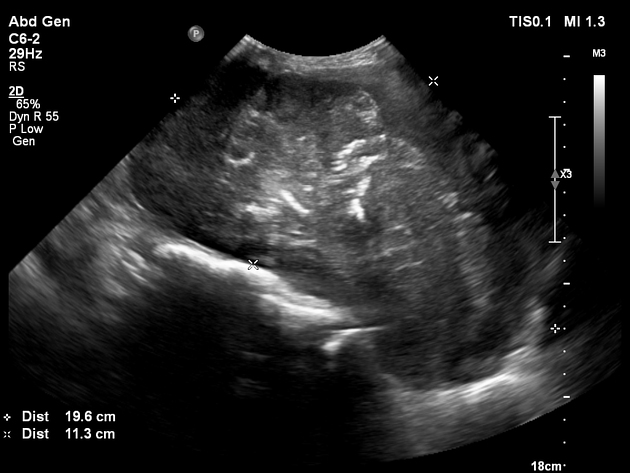
There is a large, solid, irregular, lobulated, septated, central, abdominopelvic mass that is inseparable from the uterus. There is blood flow within the identified septa. There is intralesional speckled calcification. The ovaries are not identified. There is moderate left hydronephrosis and mild right hydronephrosis. There is no ascites. No hepatic metastases visualized.
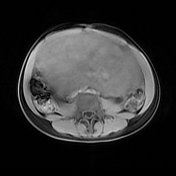
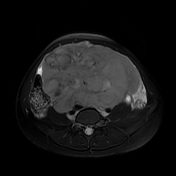
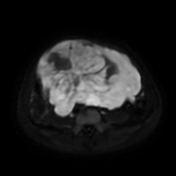
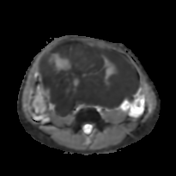

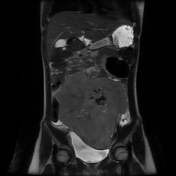
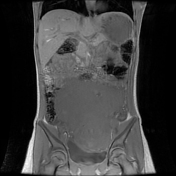
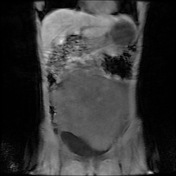
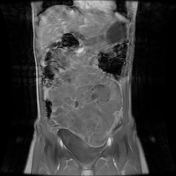
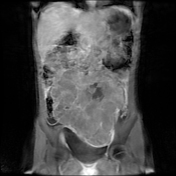

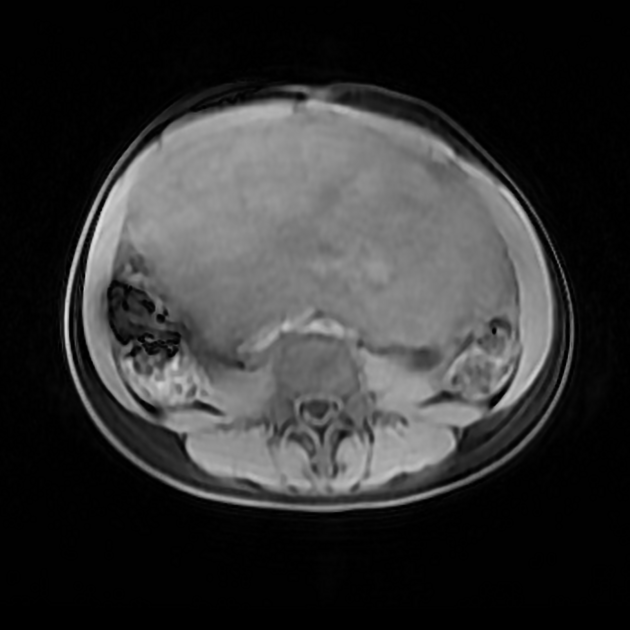
There is a large, solid, lobulated, irregular, septated, heterogeneous, predominantly solid mass arising in the left adnexa and extending to the upper abdomen. The approximate size of the mass is 19.2 x 17.3 x 16.5 cm (CC x AP x TV). There is evidence of cystic breakdown and background calcification. The mass demonstrates mild heterogeneous enhancement on post-contrast imaging. There is a mixed appearance on diffusion imaging with significantly reduced ADC mapping of the predominant solid components. The lesion appears inseparable from the uterus with an eccentric uterine cavity demonstrated posterolaterally right-sided. Inconspicuous ovaries bilaterally.
There is evidence of extrinsic ureteric compression bilaterally with consequent moderate to severe left hydronephrosis and hydroureter and mild right hydronephrosis and hydroureter.
Displaced but non-obstructed bowel loops. Antero-inferiorly displaced bladder present.
There is minimal ascites. There are no osseous or hepatic metastases.



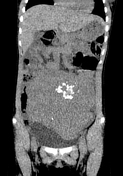

Non-contrast CT imaging of the abdomen and pelvis confirms a large, predominantly solid, lobular mass lesion arising from the left adnexa and extending superiorly to a level above the umbilicus. Speckled calcifications are present. Scattered areas of cystic breakdown are appreciated, especially within the right superior pole of the mass. The uterus and ovaries are poorly identified. There is contrast excretion (gadolinium) within the right renal tract and faint contrast within the left kidney, with mild right and moderate left renal tract obstruction. There are displaced but non-obstructed bowel loops. There is no ascites. There are obvious hepatic metastases on non-contrast CT imaging. There are no documented bone metastases.




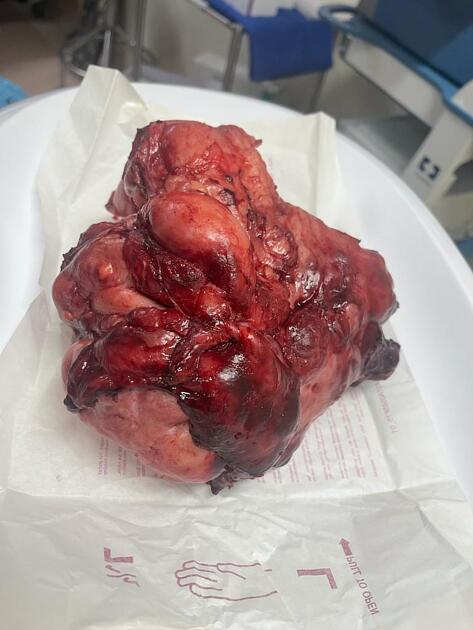
The gross appearance of the resected mass and inseparable uterus including the right ovary. The excised specimen weighed 1.825 kilograms.
The histopathology confirmed an ovarian dysgerminoma, without any mixed germ cell tumor.
Immunohistochemistry:
PLAP- positive
OCT3/4- diffusely positive
CD117- diffusely positive
EMA- negative
CD30- negative within the tumor cells
Case Discussion
An example of a histopathologically proven ovarian dysgerminoma arising from the right ovary in a young prepubertal patient. In this instance, the uterus and ovaries were poorly delineated in all imaging studies, and a differential diagnosis of uterine rhabdomyosarcoma and ovarian mass lesions, including ovarian fibrothecoma, was considered.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.