Aspiration is unintended inhalation of fluid or solid material. The location is commonly posterior, influenced by gravity. The consequences vary and and include atelectasis, inflammation (pneumonitis or bronchiolitis), aspiration pneumonia (often anaerobic bacteria), scarring and bronchiectasis 3.
On this page:
Terminology
The term aspiration is used if material passes below the level of the vocal folds, i.e. subglottic. If material enters the larynx but remains above the vocal folds, this is called penetration.
Pathology
The swallowing act is a well-coordinated and complex process, which, once initiated, is largely involuntary. The timely elevation of the hyoid and larynx, as well as the posteroinferior tilt of the epiglottis, ensure that the laryngeal aditus is closed as the bolus of food/drink passes.
Etiology
Macro-aspiration can occur during eating or drinking and may occasionally occur in healthy individuals (e.g. when simultaneously talking and eating) and should provoke a vigorous cough reflex. Numerous pathologies can cause laryngopharyngeal dysfunction that predisposes to recurrent aspirations:
neurological insults (e.g. stroke, palsy of cranial nerves IX, X and XII or neurodegenerative diseases) can result in impaired coordination of deglutition
alterations of normal anatomy (e.g. tumor, after operation or radiation) and impaired pharyngoesophageal clearance are predisposing factors
unconscious patients are prone to aspiration of vomitus because of subdued/absent defensive reflexes
foreign body aspiration: frequently happens in toddlers
meconium aspiration: a complication in newborns
tracheoesophageal fistula: rare cause of aspiration in infants
Radiographic features
Aspirated material and consequential lung pathology can be visualized with chest x-ray or CT. Videofluoroscopic swallow studies allow direct observation and analysis of the aspiration event. Small volume or slow aspiration can be diagnosed with nuclear medicine SPECT.
Plain radiograph / CT
Findings are discussed in the article on pulmonary aspiration diseases.
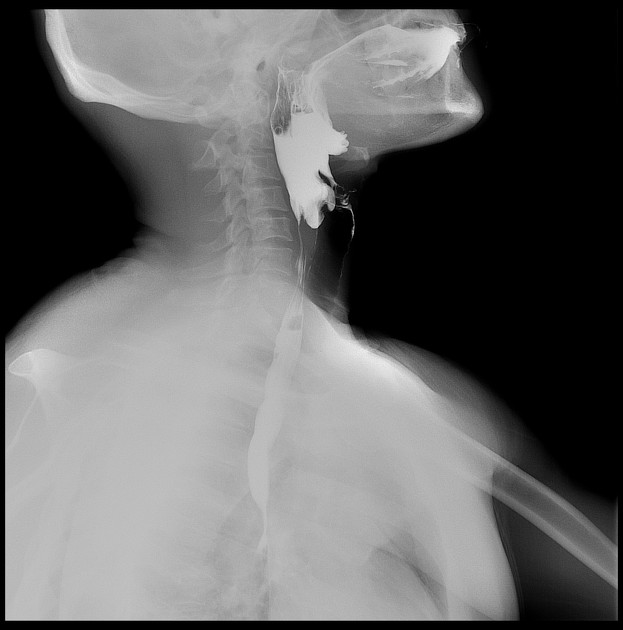
Fluoroscopy
A videofluoroscopic swallow study can visualize the timing, mechanism and extent of aspiration.
-
predeglutitive: aspiration occurs before the swallowing reflex is initiated
lack of bolus control: dorsal leaking, delayed initiation of swallowing reflex
-
intradeglutitive: aspiration occurs during the swallowing act
insufficient larynx closure: reduced or delayed elevation of hyoid/larynx, incomplete epiglottic tilt, postoperative status, impaired pharyngeal clearance
-
postdeglutitive: aspiration occurs after the main bolus has passed the pharynx
associated with pharyngeal retentions
The severity of aspiration can be graded using the penetration-aspiration scale.1
If a patient aspirates, one important factor is the presence of a sufficient cough reflex. The absence of an appropriate cough reflex (indicating "silent aspiration") may be associated with higher morbidity 2.
See also barium aspiration.
Choice of contrast medium
If a patient is at risk of aspiration the study should be performed with low osmolar water-soluble contrast medium (e.g. Omnipaque, Gastromiro). High osmolar contrast media (e.g. Gastrografin) are contraindicated due to the significant risk of flash pulmonary edema. Though aspiration of small amounts of barium sulfate contrast medium is generally not regarded harmful it can cause pulmonary baritosis and aspiration of larger amounts may lead to death.
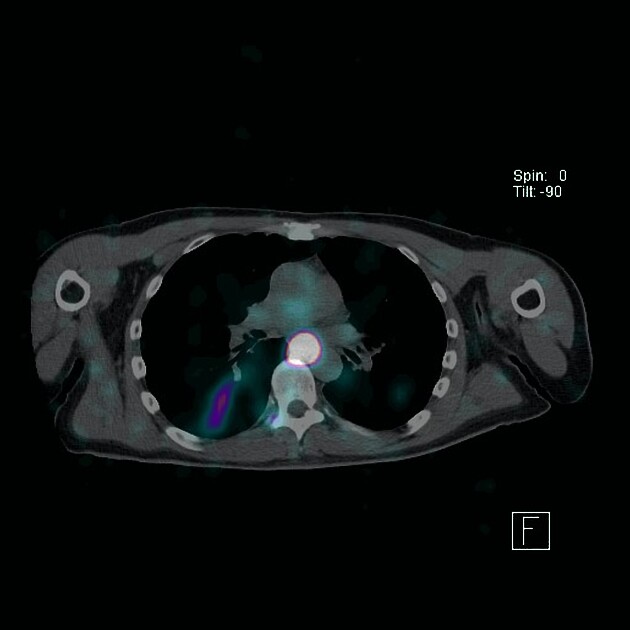
Nuclear medicine
A SPECT study performed following a small amount of radiotracer administration to the back of the oral cavity has high sensitivity for detecting salivary aspiration. Advantages of a SPECT include:
low dose (good for pediatric patients)
no need to swallow large volumes of contrast
patients can be imaged over hours to increase sensitivity





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.